


Abstract
Background Low back pain (LBP) is a globally prevalent condition, often attributed to lumbar disc herniation (LDH). Transforaminal percutaneous endoscopic discectomy (TPED) is a minimally invasive surgical approach for LDH, offering distinct advantages. This study aimed to assess the progression of pain in patients who underwent TPED in Kenya, with a focus on the impact of pre-existing factors.
Methods This retrospective study included 610 patients from the Mediheal Group of Hospitals who underwent TPED between January 2018 and December 2022. Data were collected from medical records, direct patient interactions, and telephone interviews. Statistical analyses, including repeated measures analysis of variance, correlation coefficients, and t tests, were used to examine pain progression and factors influencing outcomes.
Results Among the 610 included patients, all reported LBP and 87.9% reported leg pain. TPED resulted in significant pain reduction (P < 0.001) for both LBP and leg pain, with sustained improvement over 1 year. Factors such as age, body mass index, and duration of pain correlated with pain outcomes. No significant impact of comorbidities on pre- or postoperative pain was observed. Its retrospective design and the absence of a control group limit the strength of causal inferences.
Conclusions TPED is an effective treatment for LBP and leg pain in Kenyan patients with LDH. Pain improvement was sustained over 1 year after performing TPED, and pre-existing factors influenced outcomes. This study provides valuable insights into TPED outcomes, contributing to the understanding of LDH management in diverse populations.
Introduction
Globally, low back pain (LBP) is one of the most common symptoms that an individual encounters. Almost 80% of people suffer from at least 1 episode of LBP during their lifetimes.1 Lumbar disc herniation (LDH) is one of the most common differential diagnoses of LBP.2 The lumbar spine is made up of 5 vertebrae and intervertebral discs that give rise to a lordotic curve. These discs, in conjunction with the laminae, pedicles, and articular processes of neighboring vertebrae, form the channel through which the spinal nerves emerge. These intervertebral discs are composed of 3 parts: an inner nucleus pulposus, an outer annulus fibrosus, and cartilaginous endplates that secure the disc to its adjacent vertebrae.3 The main indications of LDH include radicular pain, sensory irregularities, and muscle weakness affecting 1 or more of the lumbosacral nerve roots.4,5 Additionally, signs such as localized muscle weakness, limited ability to bend the trunk, and exacerbation of leg pain (LP) during activities such as straining, coughing, and sneezing are suggestive of LDH.4,5 Patients often complain of intensified pain when seated, a situation known to raise disc pressure by approximately 40%.6 While microdiscectomy is commonly regarded as the preferred approach of surgery in patients suffering from LDH, the demand for less invasive methods and advancements in optical and surgical instrument technology have resulted in the adoption of transforaminal percutaneous endoscopic discectomy (TPED) through the Transforaminal Endoscopic Spine System technique.7–9 TPED, which is performed under local anesthesia and mild sedation, offers several benefits, including the ability to directly observe the underlying issue, minimizing damage to soft tissue, decreasing blood loss, expediting the recovery process, and safeguarding the neighboring anatomical structures. When performed by a skilled spine surgeon who adheres to specific protocols, it can prove to be an efficient and effective surgical method.7 All patients undergo continuous monitoring of vital signs such as blood pressure, pulse rate, oxygen saturation, and electrocardiographic signals throughout TPED. Following the surgery, patients spend the next hour in the monitoring area and are subsequently encouraged to become mobile. They remain hospitalized on the day of the procedure and are typically discharged on the first day after the operation. Patients are usually scheduled for a follow-up appointment 6 weeks after the surgery, with subsequent follow-up appointments usually scheduled at intervals of 6 weeks, 3 months, 6 months, and 1 year after the surgery.7,9,10 A review of the existing literature revealed that there were no studies assessing the results and progression of pain in patients who had undergone TPED in Kenya. The aim of our study is to discover the progression of pain in patients who underwent TPED at the Mediheal Group of Hospitals in Kenya and to examine the effect of pre-existing factors on these patients.
Materials and Methods
Study Design
Our study is a single-center, retrospective, observational study that included all patients who underwent TPED at the Mediheal Group of Hospitals in Kenya.
Patients
All patients who underwent TPED at the Mediheal Group of Hospitals between 1 January 2018 to the end of December 2022 were included in the study. However, a total of 47 patients were excluded from the study due to difficulties in communication that hindered data collection. There was no minimum or maximum age limit.
Surgeon
All TPED procedures of our study were performed by the same surgeon with assistance from a designated member of the surgical team. After surgery, patients stayed in the hospital and were monitored for a few days per standard procedures in Kenya at the Mediheal Group of Hospitals.
Data Collection and Analysis
For eligible patients, data were collected from multiple sources. Information was extracted from patients’ medical records, obtained directly from the patients during follow-up visits, or gathered via telephone interviews. This comprehensive data collection approach included the assessment of comorbidities.
Before commencing data analysis, range checks were implemented and data errors were rectified. Missing data were inputted using statistical methods.
IBM SPSS Version 23 (IBM Corp, USA) was used for the analysis of LBP and LP data. Descriptive statistics for categorical variables were presented as frequencies and percentages, while continuous variables were expressed as mean ± SD. Repeated measures analysis of variance was utilized to explore the impact of the surgical procedure on LBP and LP data. The association between preoperative pain scores and postoperative pain scores was assessed using the nonparametric Spearman’s correlation coefficient, given that the data were ranked on a scale of 0 to 10. Student independent t test and 1-way analysis of variance were used to detect any differences in pain scores based on basic characteristics (eg, gender, comorbidities). The complications variable was excluded from the analysis because only 8 patients reported complications. A significance level of P < 0.05 was set to establish statistical significance.
Results
A total of 610 patients were included in our study. All 610 participants reported LBP, and 536 also reported LP. A 10-point visual analog scale (VAS) was employed to assess LBP under 2 conditions: during motion and in a state of numbness/tingling. All participants underwent TPED and were followed up for 1 year. VAS data were collected once at before TPED and 6 times after the procedure at 3 days, 1 month, 3 months, 6 months, 9 months, and 1 year. Table 1 presents the categorical characteristics of the study participants.
Patient characteristics (categorical variables).
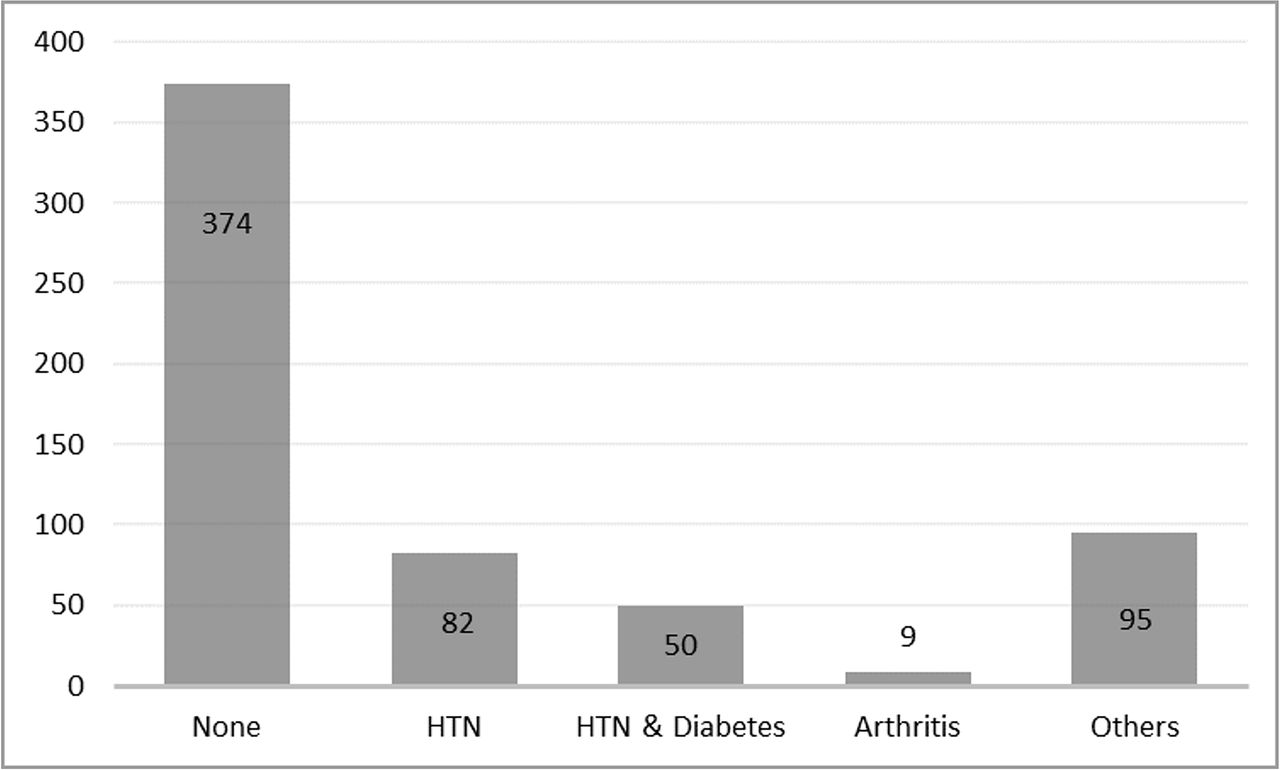
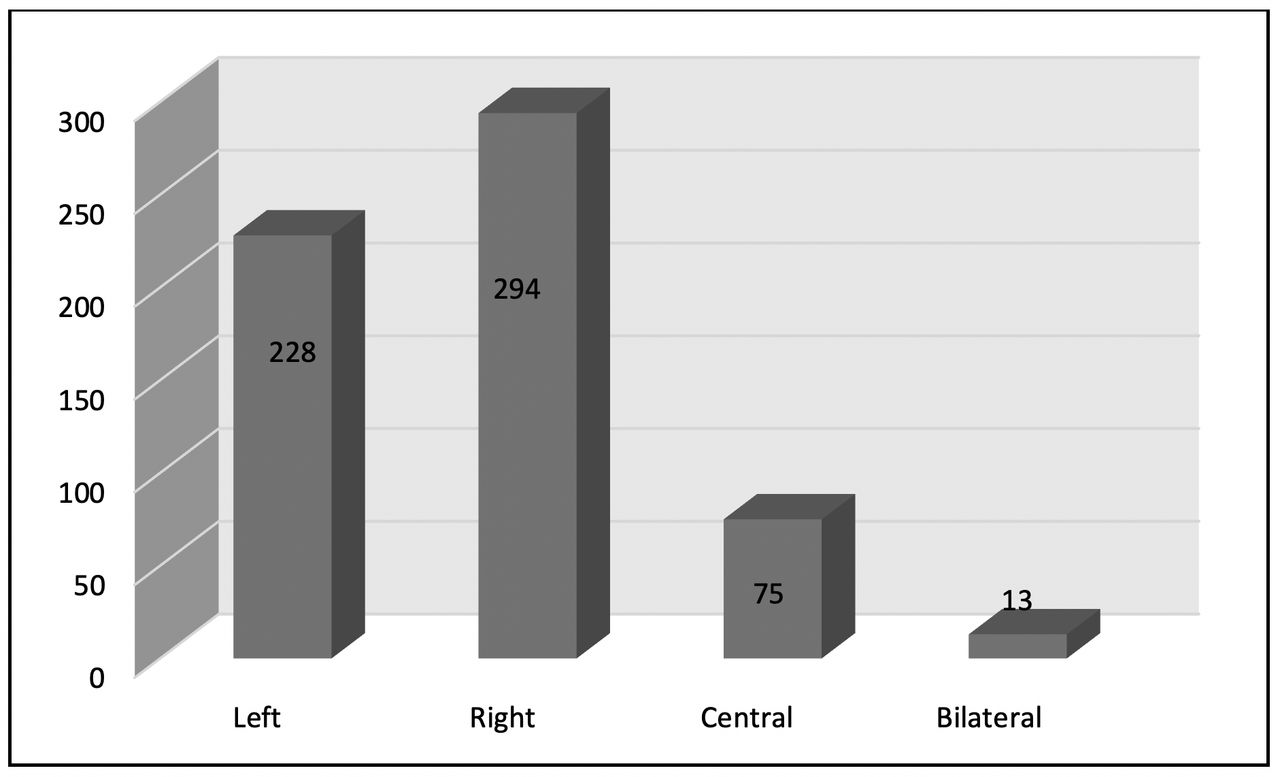
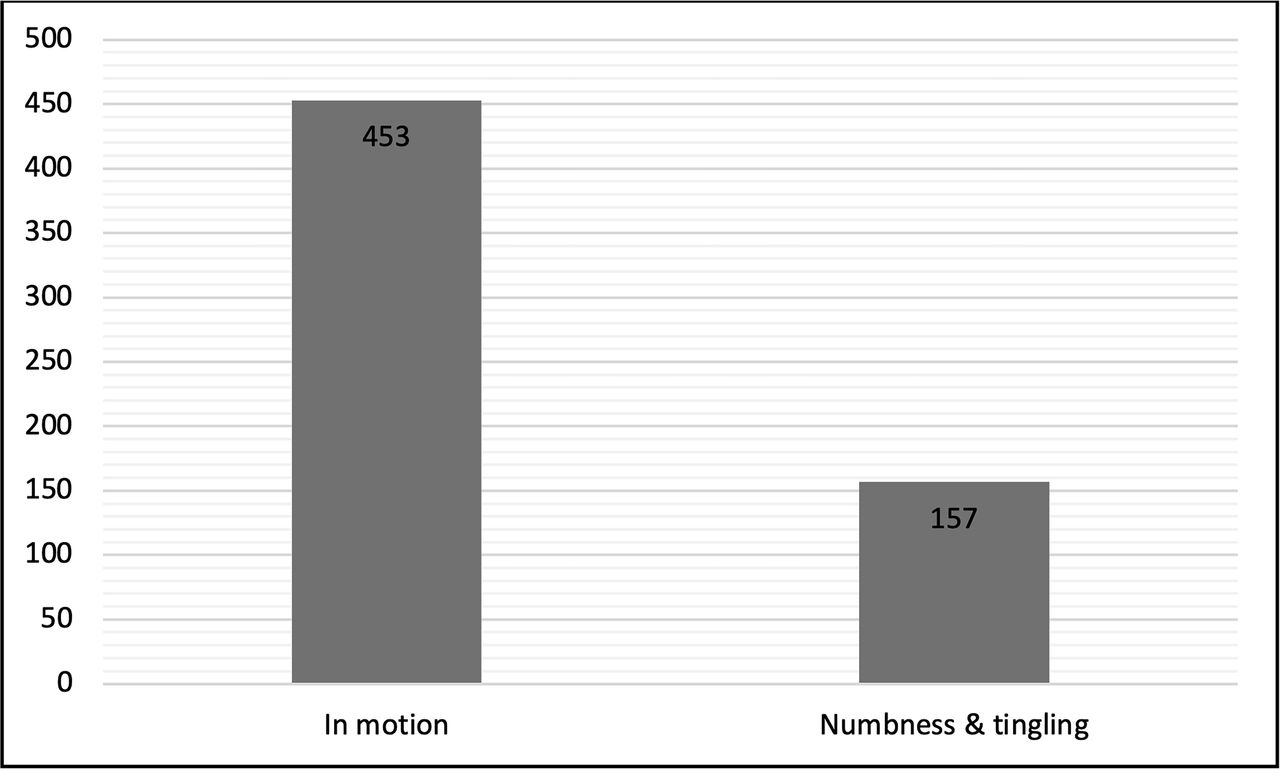
Most participants were women (65.7%), and the majority had no comorbidities (61.3%). Most of the operations were performed on the right side of patients’ bodies (48.2%), although a substantial number of patients’ operations were on their left side (37.4%). A total of 10.3% of the participants were smokers, and 17.0% of the patients reported alcohol consumption. All patients had LBP and 87.9% reported LP. The distribution of neurological symptoms showed that 74.3% of patients experienced symptoms during motion, while 25.7% reported numbness and tingling. After undergoing surgery, 8 patients experienced complications, which were minor, such as infection, difficulty in walking, difficulty in moving 1 of the legs, and foot drop.
Table 2 provides information on continuous variables regarding the characteristics of study participants.
Patient’s characteristics (continuous variables).
The age of participants ranged from 16 to 91 years, with a mean age of 50.25 years (SD = 2.43). The mean body mass index (BMI) was 29.58 (SD = 4.77), and the mean duration of pain was 3.88 years (SD = 2.43). Preprocedure pain scores ranged from 5 to 10, with a mean score of 7.63 (SD = 0.94). Figures 1–3 provide graphical representations of patient comorbidities, site of the procedure, and distribution of neurological symptoms. All operations were performed under various levels of conscious sedation in addition to local anesthetic injections. Patients were placed in prone positions. The surgeon depended on direct communication with patients to monitor their nervous system. No other neuromonitoring system or method was used. A total of 536 patients (87.9%) underwent operations on a single site (level 1), 63 (10.3%) underwent operations in 2 sites or (level 2), and 11 (1.8%) were operated on in 3 different sites (level 3).

Distribution of comorbidities. Abbreviation: HTN, hypertension

Distribution of site of procedure.

Distribution of neurological symptoms.
Age showed significant positive relationships with pain (R = 0.395. P < 0.001), preoperative pain (R = 0.083, P < 0.05), and 1-year postoperative pain (R = 0.092, P < 0.05). BMI also displayed significant positive relationships with the duration of pain (R = 0.179, P < 0.001), preoperative pain score (R = 0.128, P < 0.05), and postoperative pain score (R = 0.195, P < 0.001). A significant correlation was observed between the duration of pain and length of stay in the hospital (R = 0.153, P < 0.001). No significant correlations were found between smoking and pain severity or between consumption of alcohol and pain severity. Table 3 presents the changes in pain severity over time using the VAS.
Pain severity-predicted mean on repeated measures.
Patients reported significant improvements in both LBP and LP 3 days after the procedure (P < 0.001), as the mean pain score decreased from 7.63 and 7.67 points for LBP and LP, respectively, to 2.45 and 2.49 points after 1 year following TPED. These improvements were sustained at each time point throughout the 1-year follow-up. Figure 4 shows the comparison of changes in LBP and LP.

Comparison of changes in low back pain (LBP) and leg pain LP). The time points illustrated, from left to right, are as follows: before the procedure and 3 days, 1 month, 3 months, 6 months, 9 months, and 1 year after the procedure.
Patients undergoing the operation during the first 3 years of our study (group 1) had significantly lower average VAS pain scores after 6 months, 9 months, and 1 year of being operated (2.86, 2.52, and 2.34, respectively) compared with patients who had their surgery in the last 3 years of the study (group 2; 3.14, 2.76, and 2.57, respectively). Table 4 shows the comparison of VAS LBP scores between the 2 groups. However, we cannot exclude the contribution of patients’ demographic, biological, and psychosocial factors to the severity of pain. The incidence of complications was more prevalent in group 1 when compared with those in group 2, which might be related to the gained experience of the primary surgeon. However, the small number of complications cannot guarantee the statistical significance of these findings.
Comparison of VAS low back pain scores between Group 1 and Group 2 participants (N = 610).
Discussion
In this retrospective study, we meticulously examined the outcomes of TPED in a cohort of 610 patients. Of these participants, all 610 reported experiencing LBP, and 536 participants also reported concurrent LP. This study uncovered several noteworthy relationships and correlations.
Age displayed significant positive correlations with the duration of pain, preoperative pain scores, and postoperative pain scores throughout the follow-up data collection period. This finding indicates that older participants were more likely to suffer from additional pain compared with those who were younger. Similarly, BMI demonstrated significant positive correlations with the duration of pain, preoperative pain scores, and postoperative pain scores. Patients with higher BMI scores were more likely to suffer from additional pain, and their recovery period was longer. Furthermore, a correlation emerged between the duration of pain and length of hospital stay, illuminating the potential impact of pain duration on the postoperative recovery process.
The investigation into pain severity, using the VAS scale, provided vital insights into the outcomes of TPED. Participants experienced substantial improvements in both LBP and LP as early as 3 days after the procedure, and these improvements were sustained throughout the 1-year follow-up period. The noteworthy reduction in mean pain scores from 7.63 to 2.45 for LBP and from 7.67 to 2.49 for LP underscores the effectiveness of TPED in mitigating pain. Our study shows that after undergoing TPED, participants on average felt 67.9% less LBP and 67.5% less LP. These findings align with previous studies that have demonstrated the efficacy of TPED in managing LBP and LP. Two similar studies conducted in China and Japan showed that the VAS score for participants decreased from 5.10 and 8.64 preoperatively to 2.00 and 1.55 one year after performing TPED, respectively.11,12 Another study from China showed that the VAS score for LBP decreased from 3.90 preoperatively to 0.50 one year after performing TPED. Similarly, the VAS score for LP decreased from 5.50 to 0.60 in the same study.13 A study performed in Malaysia showed a significant decrease in VAS of patients who underwent TPED. The VAS scores decreased from 6.30 before the operation to 2.00 one year after TPED was performed.14 Similar results were also obtained in a study performed in Egypt where LBP and LP were significantly reduced (87.0% pain reduction) after 6 months of performing TPED.15 Moreover, a systematic review that included 39 previous international studies also reported significant overall pain reduction for patients who underwent TPED.16 Our results underscore the positive impact of TPED as a minimally invasive surgical approach, offering substantial pain relief and enhancing the overall quality of life for patients suffering from LDH.
While this study offers valuable insights, it is not without limitations. Its retrospective design and the absence of a control group limit the strength of causal inferences. Future research should explore prospective studies with larger cohorts, taking into account a wider array of variables, to provide more comprehensive insights into the long-term effects of TPED on LBP and LP outcomes. Our plan of action was to follow up with the patients for a longer period to assess the long-term outcomes of TPED; however, this was not feasible as we lost communication with many patients, and we faced a lot of difficulty contacting with the rest of the patients. Further communication could have improved the relevance and applicability of our study.
Conclusion
This retrospective analysis provides comprehensive insights into the outcomes of TPED for LBP and LP. This study highlights the significant reduction in pain scores following TPED, emphasizing its efficacy as a therapeutic intervention. Furthermore, age and BMI emerged as critical factors influencing pain outcomes, reinforcing the importance of considering these variables in patient management.
Footnotes
Funding No funding was received for this study.
Disclosures The authors report no financial or other conflicts of interest related to this study.
Author Contributions All authors whose names appear on the submission made substantial contributions to the conception or design of the study. Dr. A. Kaki assisted in screening and obtaining publications for systematic review. All authors worked collaboratively to write the first draft of the manuscript. All authors contributed to the validation and review of the manuscript. All authors critically reviewed the results and approved the final version of the manuscript.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.