


Abstract
Background Cervical radiculopathy is a spine ailment frequently requiring surgical decompression via anterior cervical discectomy and fusion (ACDF) or posterior foraminotomy/discectomy. While endoscopic posterior foraminotomy/discectomy is gaining popularity, its financial impact remains understudied despite equivalent randomized long-term outcomes to ACDF. In a cohort of patients undergoing ACDF vs endoscopic posterior cervical foraminotomy/discectomy, we sought to compare the total cost of the surgical episode while confirming an equivalent safety profile and perioperative outcomes.
Methods A single-center retrospective cohort study of patients with unilateral cervical radiculopathy undergoing ACDF or endoscopic cervical foraminotomy between 2018 and 2023 was undertaken. Primary outcomes included the total cost of care for the initial surgical episode (not charges or reimbursement). Perioperative variables and neurological recovery were recorded. Multivariable analysis tested age, body mass index, race, gender, insurance type, operative time, and length of stay.
Results A total of 38 ACDF and 17 endoscopic foraminotomy/discectomy operations were performed. All patients underwent single-level surgery except for 2 two-level endoscopic decompressions. No differences were found in baseline characteristics and symptom length except for younger age (46.8 ± 9.4 vs 57.6 ± 10.3, P = 0.002) and more smokers (18.4% vs 11.8%, P = 0.043) in the ACDF group. Actual hospital costs for the episode of surgical care were markedly higher in the ACDF cohort (mean ±95% CI; $27,782 ± $2011 vs $10,103 ± $720, P < 0.001) driven by the ACDF approach (β = $17,723, P < 0.001) on multivariable analysis. On sensitivity analysis, ACDF was never cost-efficient compared with endoscopic foraminotomy, and endoscopic failure rates of 64% were required for break-even cost. ACDF was associated with significantly longer operative time (167.7 ± 22.0 vs 142.7 ± 27.4 minutes, P < 0.001) and length of stay (1.1 ± 0.5 vs 0.1 ± 0.2 days, P < 0.001). No significant difference was found regarding 90-day neurological improvement, readmission, reoperation, or complications.
Conclusion Compared with patients treated with a single-level ACDF for unilateral cervical radiculopathy, endoscopic posterior cervical foraminotomy/discectomy can achieve a similar safety profile, pain relief, and neurological recovery at considerably less cost. These findings may help patients and surgeons revisit offering the posterior cervical foraminotomy/discectomy utilizing endoscopic techniques.
Clinical Relevance Endoscopic posterior cervical foraminotomy/discectomy offers comparable safety, pain relief, and neurological recovery to traditional methods but at a significantly lower cost.
Level of Evidence 3.
Introduction
Cervical radiculopathy is typically caused by paramedian or lateral compression from bulging discs or bony compression either anteriorly from the uncovertebral joint or posteriorly from the facet, causing severe pain extending to the arms, shoulders, chest, and upper back.1 Overall bony compression is far less likely to be managed conservatively compared with disc rupture. While 90% of cervical radiculopathies resolve with conservative management, 10% require surgical intervention.2
Surgical options for cervical radiculopathy include an anterior cervical discectomy and fusion (ACDF) with possible further foraminal decompression for direct decompression of lateral stenosis or posterior cervical foraminotomy/discectomy.3–5 A clinical equipoise exists between the 2 approaches for isolated, unilateral cervical radiculopathy, with no difference in outcomes at 5 years in a large Swedish cohort.6 The ACDF procedure is remarkable for minimal postoperative pain, early discharge, and durable long-term results. However, fusion is associated with a higher risk of adjacent-level disease and higher implant costs. While complications are few, dysphagia and hoarse voice are common risks of the anterior approach. The posterior foraminotomy obviates the need for a fusion but has traditionally been associated with more postoperative neck pain due to muscle retraction.7 In addition, the posterior operation is often hindered by a venous plexus around the nerve root that reduces visibility, and soft disc removal requires considerable nerve root retraction.8,9
Advances in minimally invasive and endoscopic spine surgery have allowed posterior cervical foraminotomy/discectomy to become less invasive with far less muscle mobilization, and the endoscopic approach may considerably aid visualization.10 These patients are often treated in outpatient settings and are frequently discharged home the same day with far less neck pain than the open posterior foraminotomy. Overall, literature has shown similar clinical outcomes between open posterior cervical foraminotomy/discectomy, tubular/minimally invasive foraminotomy/discectomy, and full-endoscopic posterior cervical foraminotomy/discectomy compared with each other or ACDF.11–15 Full endoscopic foraminotomy/discectomy has several advantages over tubular or microendoscopic techniques, namely, much smaller muscle dissection (6–8 mm endoscope vs 16+ mm tubes), continuous saline irrigation that improves visualization and controls venous bleeding, and improved angle of treatment allowing optimal balance between decompression and facet preservation.10–12,16 The obvious advantages over ACDF include sparing the implant costs and eliminating the risks of the anterior cervical approach, namely dysphagia and motion limitation.
While a cost-analysis comparing ACDF and tubular cervical foraminotomy/discectomy has been previously published, the literature lacks studies comparing ACDF and full endoscopic foraminotomies/discectomies.17 In a cohort of patients undergoing ACDF vs endoscopic posterior cervical foraminotomy/discectomy for isolated, unilateral cervical radiculopathy, we sought to compare the total cost of the surgical episode while confirming an equivalent safety profile and perioperative outcomes.
Methods
Study Design
A single-center, retrospective, cohort study using prospectively collected data of patients undergoing surgical treatment for unilateral cervical radiculopathy due to degenerative spine disease between 2018 and 2023. Institutional review board (IRB) approval was obtained for this study (IRB#230293).
Patient Population
Inclusion criteria were adults undergoing primary, elective ACDF or endoscopic posterior cervical foraminotomy/discectomy for unilateral cervical radiculopathy. Patients with primary axial pain, myelopathy, instability, previous surgery, trauma, tumor, multilevel discectomy, corpectomy, concomitant cervical or thoracolumbar surgery, or prior cervicothoracic fusion were excluded.
Exposure Variable
The primary exposure variable was ACDF vs endoscopic posterior cervical foraminotomy/discectomy. The operative approaches are described below.
Additional exposure variables were evaluated and included basic demographics such as age, sex, race, body mass index, insurance, and comorbidities, as well as preoperative and radiographic variables, including length of symptoms, presence of disc herniation, calcification, and disc location (central, paramedian, and lateral).
Outcomes
The primary outcome was the total cost of care for the initial surgery and hospital stay using total hospital/provider costs, not charges or reimbursement. Initial surgical costs were adjusted to 2023 US dollars using the General Medical and Surgical Hospital Producer Price Index.18
Other outcomes recorded were perioperative data and neurological improvement. Perioperative outcomes included all data regarding the operation, index hospitalization, and postoperative period. Immediate postoperative data included operative time (minutes), length of stay, and opioid prescription at discharge. Six-week outcomes included readmission, reoperation, and neurological improvement. Regarding neurological outcomes, any improvement of radiculopathy symptoms was noted as a neurological improvement.
Anterior Cervical Discectomy and Fusion
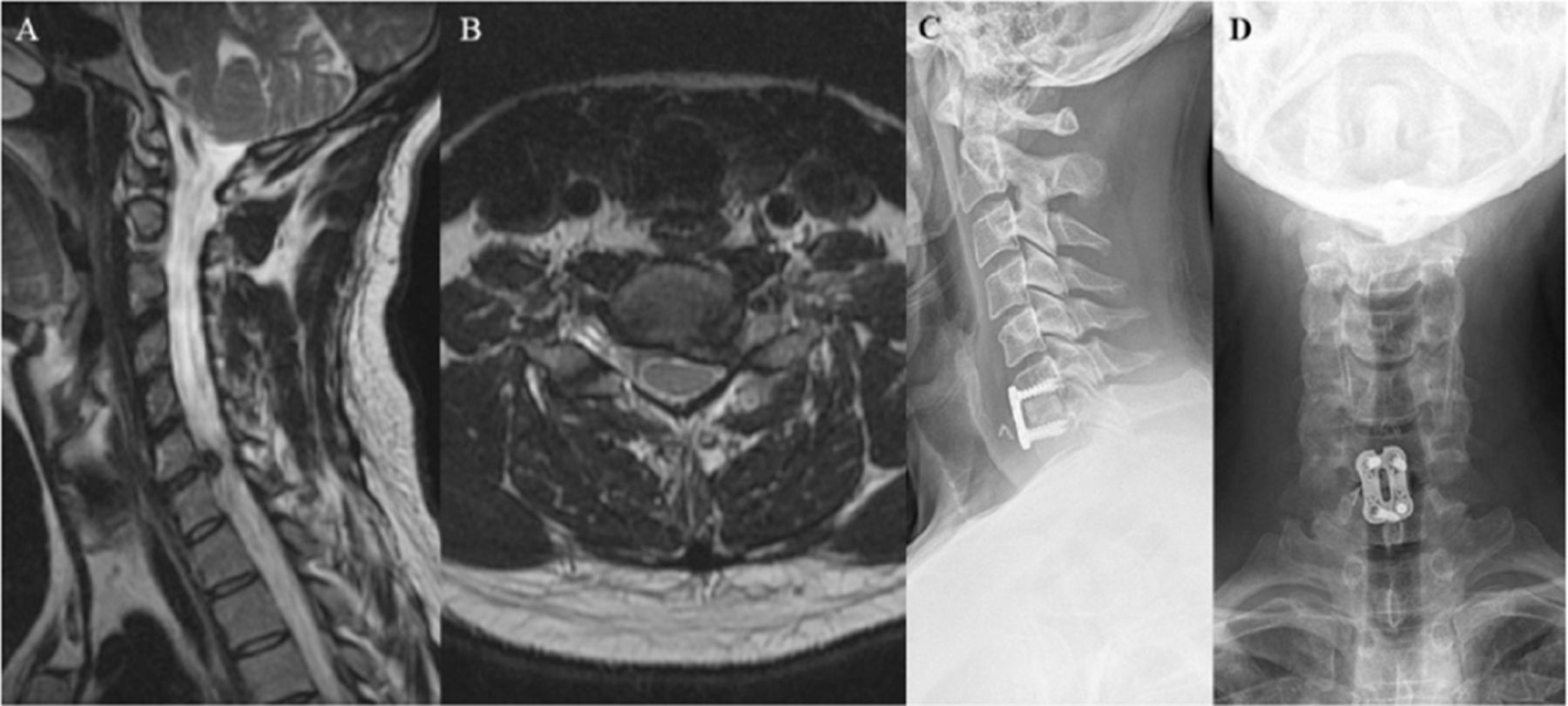
All patients were positioned supine with general anesthesia, and fluoroscopy was used for localization. The side of the approach, anterior cervical plate placement, and graft type were dependent on the surgeon’s preference and varied from allograft, polyetheretherketone, and titanium grafts. All ACDF surgeries were performed at the main academic hospital (Figure 1).

A 44-year-old man with several months of worsening left C7 radiculopathy despite conservative management was found to have large paramedian C6–C7 disc rupture seen on parasagittal (A) and axial magnetic resonance imaging (B). The patient underwent a right-side anterior cervical discectomy and fusion with structural allograft (C and D) followed by complete resolution of his radicular symptoms 5 weeks after the operation.
Endoscopic Posterior Cervical Foraminotomy/Discectomy
All surgeries were performed at the hospital-associated ambulatory surgery center (ASC) associated with the main academic hospital. Patients were positioned prone with full anesthesia, and surgery was performed using the Joimax Interlaminar Endoscopic Surgical System (iLESSYS Pro, 7.3 mm outer diameter and goes down an 8 mm cannula). Anteroposterior and lateral fluoroscopic images localized to the correct disc space level and marking of the lateral facet (lateral) and lamino-facet junction lines (medial) marked out the endoscopic trajectory toward the symptomatic level facet and adjusted medially or laterally as needed for a specific case. An 18-gauge needle was passed medial to lateral landing on the symptomatic level facet, and lidocaine was injected for preemptive analgesia. Dilators, endoscopic cannula, and the endoscope were safely parked on the medial facet at the symptomatic level, and soft tissue was cleared to reveal the V-point where the medial facet meets the lateral superior and inferior lamina. Continuous endoscopic saline irrigation at one-half of the patient’s diastolic blood pressure allowed for tissue retraction, improved visualization, and minimal blood loss. A high-speed diamond burr drill was used to remove enough of the lateral superior lamina and inferior lamina to detach the ligamentum flavum and follow the V-point into the medial facet joint line. Care was taken to preserve the ligamentum flavum laterally and to only resect as much inferior articular process as necessary to expose sufficient medial edge of the superior articular process (SAP) as it rises cranially from the leading laminar edge. Once exposed, the visible SAP was thinned with a diamond burr and removed with a Kerrison punch, followed by removal of soft tissue and ligament to reveal the decompressed exiting nerve root. The exiting nerve root was mobilized to find any symptomatic paramedian or lateral disc compression, which could be removed with a pituitary (Figure 2).10

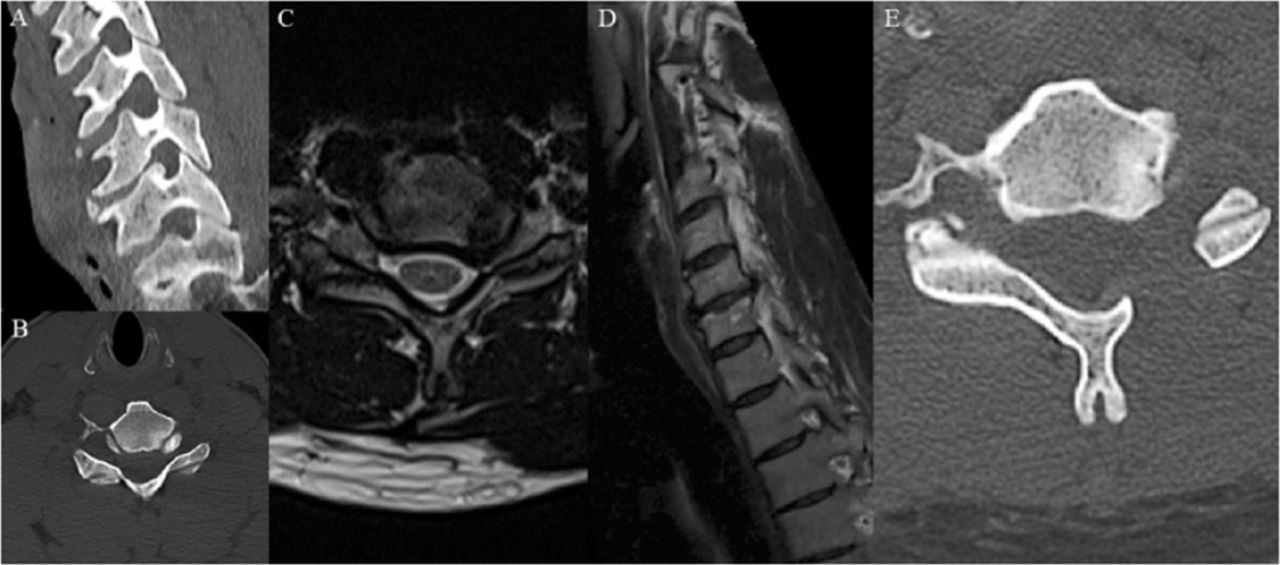
A 46-year-old man with a history of fibromyalgia and postural orthostatic tachycardia syndrome presented with 10 months of left C7 distribution radiculopathy with left triceps and wrist extension weakness despite conservative management. Preoperative imaging showing bony left C6–C7 foraminal stenosis due to uncovertebral joint hypertrophy on sagittal oblique and axial cervical spine computed tomography (A and B) with concomitant stenosis from a C6–C7 paracentral disc bulge on axial and sagittal oblique magnetic resonance imaging (C and D). The patient underwent full endoscopic left C6–C7 posterior foraminotomy (E) with subsequent improvement in C7 radicular pain and full motor recovery at 90 days postoperatively.
Statistical Analysis
Descriptive statistics were computed for all demographics and all preoperative, perioperative, and postoperative variables. Means and SDs or 95% CIs or median and interquartile ranges were reported for continuous variables, and percent frequencies were reported for the categorical variables. Histograms were generated for qualitative assessment of normality. Quantitatively, normal distribution and variance for continuous variables were assessed with the Shapiro-Wilk test, χ 2 normality test, and F test, respectively. Parametrically distributed data with equal variance were analyzed with a 2-tailed t test, while nonparametric data were compared with the Wilcoxon signed rank or Mann-Whitney U test. χ 2 or Fisher’s exact test for small samples was used for nominal data. Simple linear regression was used for univariate analysis to compare patients undergoing ACDF vs endoscopic foraminotomy/discectomy. Multivariable analysis for any variable that had a significant univariate relationship with cost at an alpha of 0.2 for either open or endoscopic surgery. Stepwise multivariable regression removed nonsignificant variables at an alpha of P < 0.05 and allowed simultaneous focus on the main drivers of cost and control of multicollinearity. General statistical analysis was performed using SPSS version 22 (IBM Inc., Chicago, Illinois). StatTools version 8.1 (Lumivero Inc., Denver, Colorado) and TreeAge Healthcare software were used to perform cost analysis, sensitivity analysis, and break-even analysis assuming all ACDF and endoscopic revisions underwent ACDF revision surgery. Post-hoc power analysis for continuous independent variables was performed for the primary outcome.19
Results
Baseline Characteristics
A total of 38 patients underwent ACDF, and 17 patients underwent endoscopic cervical foraminotomies/discectomies for unilateral cervical radiculopathy. All patients underwent single-level surgery except for 2 endoscopic patients with 2-level isolated, unilateral radiculopathies. No difference was found in baseline characteristics and symptom length, except for younger age and (46.8 ± 9.4 vs 57.6 ± 10.3, P = 0.002) and more smokers (18.4% vs 11.8%, P = 0.043) in the ACDF group. Similarly, no statistically significant difference was found in demographic variables such as sex, race, insurance status, or comorbidities (Table 1). All patients had disc herniation, with no difference in disc herniation location (P = 0.248) and duration of symptoms (P = 0.737; Table 2). No difference was found in the mean follow-up time between the 2 groups (11.5 ± 10.7 vs 7.1 ± 7.4 months, P = 0.247).
Demographics and preoperative variables.
Perioperative and postoperative outcomes.
Costs
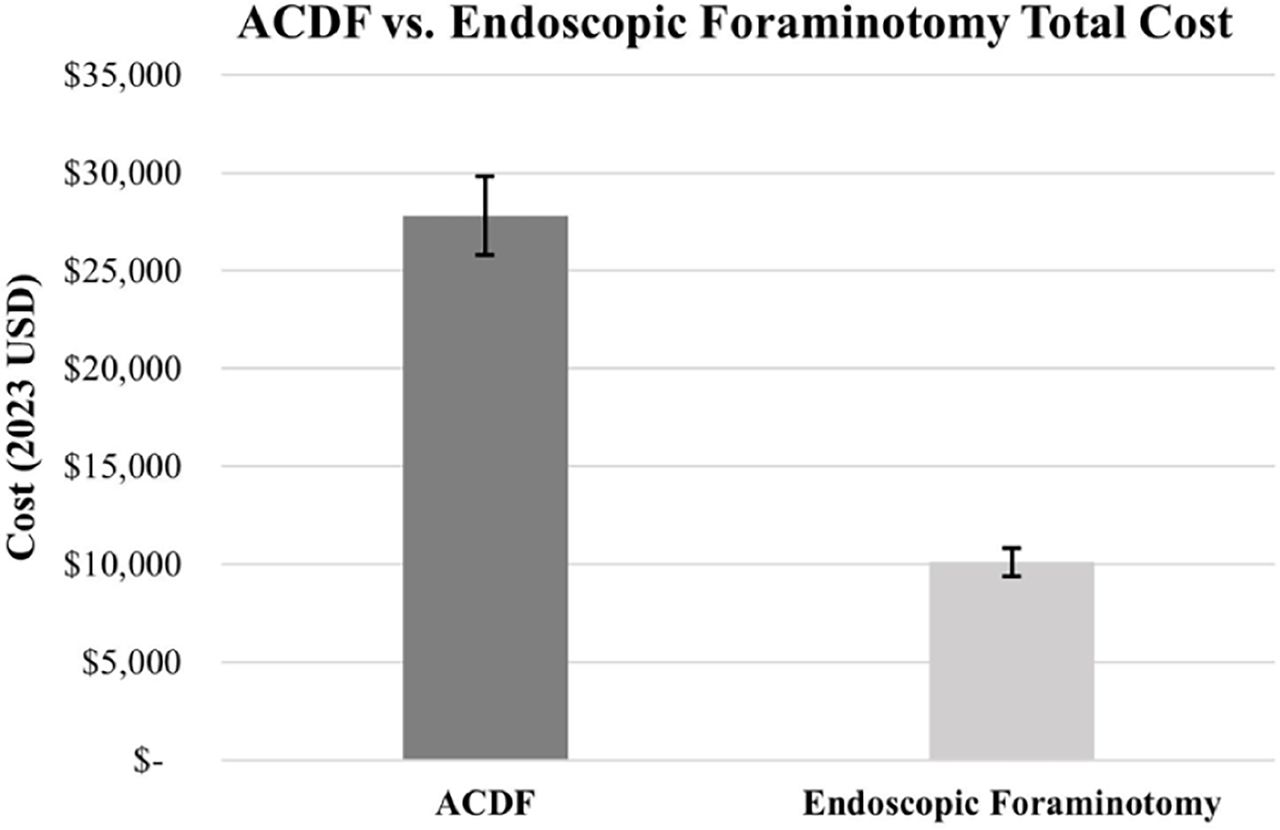
ACDF costs were 2.75× higher than endoscopic foraminotomy/discectomy (mean ±95% CI; $27,782 ± $2011 vs $10,103 ± $720, P < 0.001), significantly driven only by the ACDF approach (β = 17,723, P < 0.001) on multivariable stepwise regression analysis (Figure 3; Table 3). Multicollinearity as measured by the variance inflation factor was below the threshold of 10 requiring further investigation for interaction between independent variables.20 The study was 100% powered to examine differences in cost.

Total initial anterior cervical discectomy and fusion (ACDF) vs endoscopic foraminotomy cost (mean ± 95% CI total surgical costs for each cohort).
Univariate and multivariable drivers of cost.
Cost Sensitivity Analysis
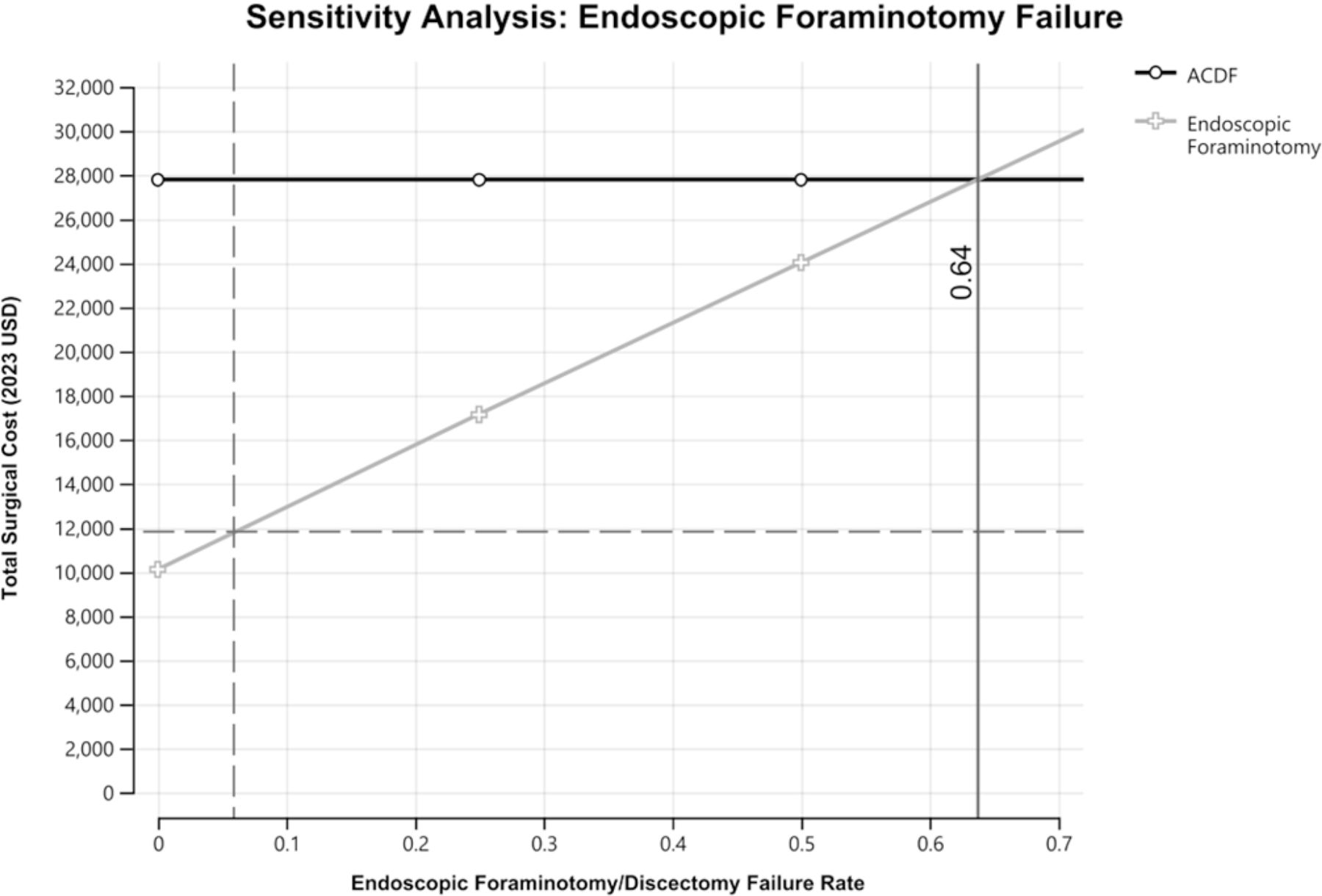
On sensitivity analysis, no variables could make ACDF cost-efficient compared with endoscopic repair, and the modeled incremental cost after including revision rates was substantially higher for ACDF (+$16,743 [$28,557 ACDF vs $11,814 endoscopic foraminotomy/discectomy]; Figure 4). Revision rates of 64% were required for break-even costs, even assuming all endoscopic revisions required an ACDF (Figure 5). Put conversely, if outpatient full endoscopic posterior foraminotomy/discectomy were the default first surgery for operative cervical radiculopathy, with ACDF reserved only for failed foraminotomies, only a 36% endoscopic foraminotomy/discectomy success rate would be required for cost equipoise with current ACDF-first pathways even assuming no ACDF revisions or complications.

Sensitivity analysis of anterior cervical discectomy and fusion (ACDF) vs endoscopic foraminotomy shows the potential impact of surgical costs and revision rates on overall cost differences between ACDF and endoscopic cervical foraminotomy ($0 on X-axis). No input variability brought ACDF costs below endoscopic cervical foraminotomy costs. Median surgical costs were used as base values with variation between the highest (gray) and lowest (black) studied costs in each variable. Revision rate base values was the percentage of each cohort undergoing revision surgery with variation tested at ±10 absolute percentage points. For sensitivity analysis, all surgical failures were eventually assumed to undergo ACDF revision. Modeled incremental cost after including revision rates was higher for ACDF (+$16,743 [$28,557 ACDF vs $11,814 endoscopic foraminotomy/discectomy]).

Break-even analysis. Univariate sensitivity analysis testing endoscopic cervical foraminotomy failure rates (x axis) against the total cost of surgical care (y axis, including revisions), showed that break-even costs between initial ACDF and endoscopic foraminotomy occurred at a 64% endoscopic foraminotomy failure rate (solid gray line, x axis). Analysis assumes no ACDF failures and that every endoscopic foraminotomy failure was ultimately treated with an ACDF. Dashed gray lines show the currently observed endoscopic foraminotomy failure rate (x axis, 5.9%) and the corresponding modeled weighted-average total endoscopic foraminotomy cost including revisions with ACDF after failure ($11,814).
Perioperative and Postoperative Outcomes
Patients undergoing ACDF had a significantly longer operative time (167.7 ± 22.0 vs 142.7 ± 27.4 min, P < 0.001), blood loss (32.2 ± 47.6 vs 9.9 ± 11.6 mL, P < 0.001), and length of stay (1.1 ± 0.5 vs 0.1 ± 0.2 days, P < 0.001; Table 2).
No significant difference was found regarding 90-day neurological improvement, readmission (0% vs 5.9%, P = 0.309), reoperation (2.6% vs 5.9%, P = 0.527), or complications (7.9% vs 0, P = 0.544). Endoscopic foraminotomy/discectomy also has a naturally low rate of postoperative opioid prescription. Furthermore, a total of 3 minor complications treated conservatively in the ACDF group were encountered. In addition, 1 major complication requiring reoperation was encountered in each group (Table 4).
Complication and revision characteristics.
Neurological Recovery
Neurological recovery was compared to ensure that each approach accomplished nerve root decompression, the primary goal for surgery. All patients in this cohort who underwent ACDF, or endoscopic cervical foraminotomies/discectomies, had a 100% rate of neurological/pain improvement (Table 2).
Discussion
Key Findings
The current study is among the first comparing ACDF vs endoscopic posterior cervical foraminotomy/discectomy in cost of care and perioperative outcomes. Preoperatively, the 2 cohorts were similar in demographics and preoperative characteristics except for younger age and higher smoking status in the ACDF cohort. Overall costs were driven by the ACDF approach on multivariable analysis, which is not surprising given the cost of implants. Due to the 2.75-times higher cost of ACDF, an endoscopic cervical foraminotomy/discectomy revision rate requiring an ACDF of 64% is required for break-even cost. Perioperatively, ACDF was associated with increased operative time and length of stay but without a statistically significant difference in 90-day (global period) reoperation, revision, or complications. The rate of improvement in neurological symptoms was identical at 100% in both groups. These results suggest that posterior cervical endoscopic foraminotomy/discectomy is a safe, effective, and far less costly surgical alternative compared with ACDF for patients with unilateral cervical radiculopathy.
Invasiveness of Posterior Cervical Endoscopic Foraminotomy
Unilateral cervical radiculopathy is commonly treated with ACDF, and the literature has shown that posterior cervical foraminotomy/discectomy is equally effective for the treatment of unilateral radiculopathy.11–15 Endoscopic posterior cervical foraminotomy/discectomy is a less invasive approach that obviates the need for a motion-limiting spinal fusion, long-term risk to adjacent segments, or risks of dysphagia and hoarseness associated with ACDF.2–5 Notably, a randomized controlled trial comparing ACDF and endoscopic foraminotomy showed equivalent outcomes at 2 years postsurgery.15
Traditional open posterior cervical foraminotomy/discectomy tends to preserve motion and directly treat posterior compression while still allowing paramedian or lateral discectomy with a downside of a higher rate of neck pain secondary to wide subperiosteal muscle dissection that disrupts the paraspinal muscles including the multifidus muscles.7 In addition, there is a rich plexus of veins that often interferes with visibility.9 Similarly, tubular or microendoscopic posterior cervical foraminotomy/discectomy is performed via larger diameter tubes and is associated with more muscle dissection, worse operative angles with less ability to undercut and preserve the medial facet and SAP, and similar struggles with venous plexus during discectomy.16 Full posterior cervical endoscopic foraminotomy/discectomy, therefore, may strike the optimal balance between direct decompression of posterior pathology and/or anterior disc bulge, with preservation of motion and both dynamic and structural stability.
Cost Comparison
Our study found that ACDF costs were 2.75 times higher than posterior cervical endoscopic foraminotomy. As the United States has drastically different cost structures than most countries, more cost-conscious, single-payer systems such as Korea have had earlier implementation and innovation of endoscopy.10 Comparing costs between single-payer systems and private, employer-based U.S. systems is difficult. Furthermore, as only a handful of U.S. spine surgeons perform endoscopic cervical foraminotomies, and many cannot access their surgical costs, these data are valuable, and we hope they will lead to larger, multicenter studies comparing the 2 approaches. Sensitivity analysis showed that no observed variation in surgical costs or revision rates allowed ACDF to become less expensive than endoscopic foraminotomy/discectomy. An excess endoscopic foraminotomy/discectomy revision rate of 64% above ACDF revision rates was required before break-even costs, far higher than observed long-term foraminotomy vs ACDF revision rates,6 and with conservative assumptions that ACDF was performed for all revisions, and there were no ACDF failures. Overall, the fact that no observed input variability could make ACDF less costly than endoscopic foraminotomy on sensitivity analysis, and that only a 36% initial endoscopic foraminotomy-first success rate would be required for cost equipoise with current ACDF-first pathways, points to a low likelihood that the results would change if studied in other settings.
Drivers of Cost
We found that the ACDF technique was the primary driver of cost compared with endoscopic posterior foraminotomy after univariate and multivariable stepwise regression that initially included body mass index, age, race, gender, insurance, length of stay, and operating room time. Additionally, overhead costs also likely play a role between the operative costs at the general hospital (ACDF) and the hospital-owned surgery center (endoscopic cervical foraminotomy/discectomy). However, implant and overhead costs likely have similar cost pressures between large academic hospitals. While there are capital overhead costs associated with the endoscopic spine equipment, these costs are comparable with the operative microscope and traditional cervical operative equipment.21 Overall, the publishing of total surgical costs that includes implant, anesthesia, professional, and overhead costs is scarce in the literature and provides a useful analysis of the: (1) actual costs that underlying total treatment costs and charges billed to patient’s/insurance and (2) differences in techniques in hospitals vs surgery centers that are not adequately assessed by only variable cost evaluation.
Limitations
The current study is not without limitations. First, the retrospective, single-center nature of the study and relatively small sample size have inherent limitations, including generalizability. Second, the cost data are only applicable to our institution, yet we would submit that the cost results are likely applicable to most similar hospital systems. These limitations are likely applicable to any U.S. study regarding endoscopy given the relative rarity of endoscopic spine surgeons in the United States and the fact that any multicenter “cost” study would likely rely on Medicare-based reimbursement that does not account for actual cost or technical nuances of endoscopic vs traditional surgery. Additionally, our study results concur with previously published literature from other countries, making the single-center generalizability outcomes data less of a concern.12,22 Our focus on significant drivers of cost with multivariable analysis makes our results more generalizable to other hospitals that likely have similar cost pressures, even if they have slightly different baseline differences in implant purchasing power or overhead costs. Overall, the significant cost difference between ACDF and endoscopic foraminotomy/discectomy, which remains unchanged after sensitivity analysis, is unlikely to substantially change if studied in other U.S. hospitals. Third, the study has a relatively short follow-up period and can only be applied to the perioperative period. Due to its minimally invasive nature, endoscopic foraminotomy patients can return to daily function rapidly with fewer postoperative follow-up visits and naturally low opioid prescription requirements. In fact, the vast majority of our endoscopic foraminotomy patients only have a single postoperative follow-up appointment in the first 90 days and are, therefore, easily lost to follow-up unless they return with recurrent symptoms. The short follow-up period and relatively small sample inhibit tracking of longer-term pain outcomes. The durability of the posterior foraminotomy/discectomy and long-term reoperation rates cannot be assessed in this study, as our results only extend to the immediate postoperative period. Fourth, opioid prescription patterns vary significantly between surgeons without direct relation to surgical invasiveness.23,24 Due to surgeon prescription variability, this study is best equipped to show that endoscopic foraminotomy/discectomy can be performed without postoperative opioids rather than to compare opioid use with ACDFs, although this would be an interesting variable in larger, longer studies. Fifth, our study compares the cost of care for endoscopic cervical foraminotomies at the hospital-associated ASC vs outpatient ACDFs performed at the main hospital, with ACDF patient’s typically spending 1 night in the hospital. Although ACDFs are now more commonly being performed at ASCs, evidence suggests that a slim majority of ACDFs are still being performed in the hospital setting.25 Regardless, the cost difference found in our study far exceeds the average hospital cost per inpatient day and is unlikely to change if studied in other settings.26 Finally, we do not have an accepted patient-reported outcome metric, which also limits our generalizability.
Conclusion
In the current study comparing the operative outcomes and cost for ACDF vs endoscopic foraminotomy for unilateral cervical radiculopathy, patients undergoing ACDF were significantly younger and had longer surgeries, more blood loss, and longer length of stay. We also found that endoscopic cervical foraminotomy is a safe, significantly less costly alternative with equivalent neurological outcomes and naturally low postoperative opioid use. These findings may help patients and surgeons seek out posterior endoscopic cervical foraminotomy/discectomy as a less costly and less invasive surgical alternative when indicated.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests Dr. Gardocki is a consultant and teaching surgeon for Joimax, a consultant for Arthrex, a teaching surgeon and consultant with royalties for Integrity Implants, and a consultant with royalties for Spineology. Dr. Zuckerman reports being an unaffiliated neurotrauma consultant for the National Football League and consultant for Medtronic. Dr. Stephens is a consultant for Nuvasive and Carbofix and receives institutional research support from Nuvasive and Stryker Spine. Dr. Abtahi received institutional research support from Stryker Spine. No other perceived conflict of interest by any of the listed authors.
Ethics Approval This study was approved by the IRB committee at Vanderbilt University Medical Center (IRB#230293). We certify that the study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.