


Abstract
Background Vertebral augmentation has recently evolved as a medical procedure for the treatment of vertebral compression fractures, the most common type of skeletal fractures related to osteoporosis.
Methods This study compared the cement leakage and filling behavior of 2 existing delivery systems (Confidence and Vertebroplastic; DePuy Spine, Raynham, MA). The Confidence system with the high viscosity cement has been recently introduced in an attempt to curtail cement leakage.
Results The comparison was performed using an established benchmark model wherein the cement leakage, filling behavior can be assessed. A double-conduit introducer needle was used to deliver the cement and to measure the intravertebral pressure while delivering the cement. There were 5 experimental groups in this study: 3 low-viscosity groups, whose cement was injected at 3.5, 6.5, and 9.5 minutes after admixing the powder and monomer, and 2 high-viscosity groups injected at 3.5 and 6.5 minutes. The mass of leaked cement generally decreased with delaying the start of the injection. Specifically, for the low-viscosity, the average smallest leakage mass obtained was 2.6 ± 1.2g when the cement was delivered at 9.5 minutes. If delivered after 3.5 minutes, the mass of cement leak was 4.0 ± 1.2g. The high-viscosity system has showed improved results in curtailing cement leakage, as compared to low-viscosity. Specifically, if injected after 3.5 and 6.5 minutes, the cement leakage amounts were 1.5 ± 1.2g and 0.92 ± 0.6g, respectively. Similarly, the uniformity of cement filling increased when the delivery was delayed and when the high-viscosity system was applied. Furthermore, there were no significance changes in the intravertebral pressures between the low- and high-viscous groups. No correlation between the leakage mass and the IV pressures was noted.
Conclusion The cement thickness and timing of delivery are key in controlling the intravertebral cement filling and physician may want to explore the use of low- or high-viscous cement for different fractures. The thickness of the cement has no significant impact on the intravertebral pressures.
In vertebral augmentation procedures, acrylic medical cement is injected through a thin cannula into a collapsed vertebra. The cement, once hardened, provides mechanical stability for the fractured bone. Though this procedure has been reported to be effective, cement leakage into the spinal canal or the cardiovascular system may lead to serious complications such as nerve compression or embolism, and, in some rare cases, possibly causing death.1–4
Significant research related to cement leakage has been already directed toward improving the visualization techniques for timely detection and thus prevention of cement leakage.1, 2 More recently, Bohner et al focused on the understanding of the flow characteristics that the cement must have to be an adequate bone augmentation material, developing the first theoretical and experimental models of cement leakage emphasizing the leakage path.4 Using a simulated vertebral model with a path of least resistance, Baroud et al showed that high-viscosity cements spread more uniformly, thus significantly reducing the risk of leakage. 3 Specifically, if the cement is injected at a thick viscous stage, it fills more uniformly and the risk of leakage is reduced because of the poor cement mobility. This approach is a preventive method.3–5
Confidence (DePuy Spine, Raynham, MA) is a spinal augmentation system, in that the cement attains high viscosity immediately after mixing and maintains it for 9 minutes at room temperature. The objective of this study was to compare the leakage and flow behavior of the highviscosity Confidence and existing low-viscosity Vertebroplastic (DePuy Spine) systems. In addition to examining the intravertebral pressure behavior, an experimental leakage model developed in a previous study3 was used to examine the filling and leakage behavior of the the high-viscosity versus low-viscosity spinal augmentation systems. The leakage model included a distinct leakage path to simulate a blood vessel and thus to trigger cement leakage. In addition to measuring the cement leakage, cement-filling patterns in the model will be quantified.7
Furthermore, the intravertebral pressure value in the simulated vertebral model will be measured using a doubleconduit introducer needle. The intravertebral pressure is formed inside the vertebral cavities while injecting the cement, due to the resistance of the bone marrow when displaced by the cement.8
Materials and methods
The leakage model proposed in the earlier study conducted by Baroud et al3 was used to investigate the filling pattern, leakage, and intravertebral pressure of the 2 systems (the newer high-viscosity and existing low-viscosity). The laboratory leakage model is made of 95% porosity aluminum open foam with similar morphological and physical characteristics similar to the osteoporotic bone. Further information regarding the laboratory leakage model characteristic is available in Baroud et al.3, 6
The whole surface of the cylindrical aluminum foam sample was covered first with a thin layer of modeling paste in such a way that all the facial pores are closed. Blocking the leakage path and the cannula channel with fitting screws is required to prevent any blocking of them during the subsequence preparation process. Each foam sample was then dipped in a bath of bone cement to simulate the vertebral shell; this step was performed twice to ensure the thickness of the layer. After the PMMA has cured, the fitting screws were removed. The foam samples were submerged in a colored water-gelatin solution that should fill all the voids inside of the foam sample. The bath was placed for 24 hours in the refrigerator at 4°C to allow the solution to gel. The gelatin is aimed to simulate the presence of bone marrow.
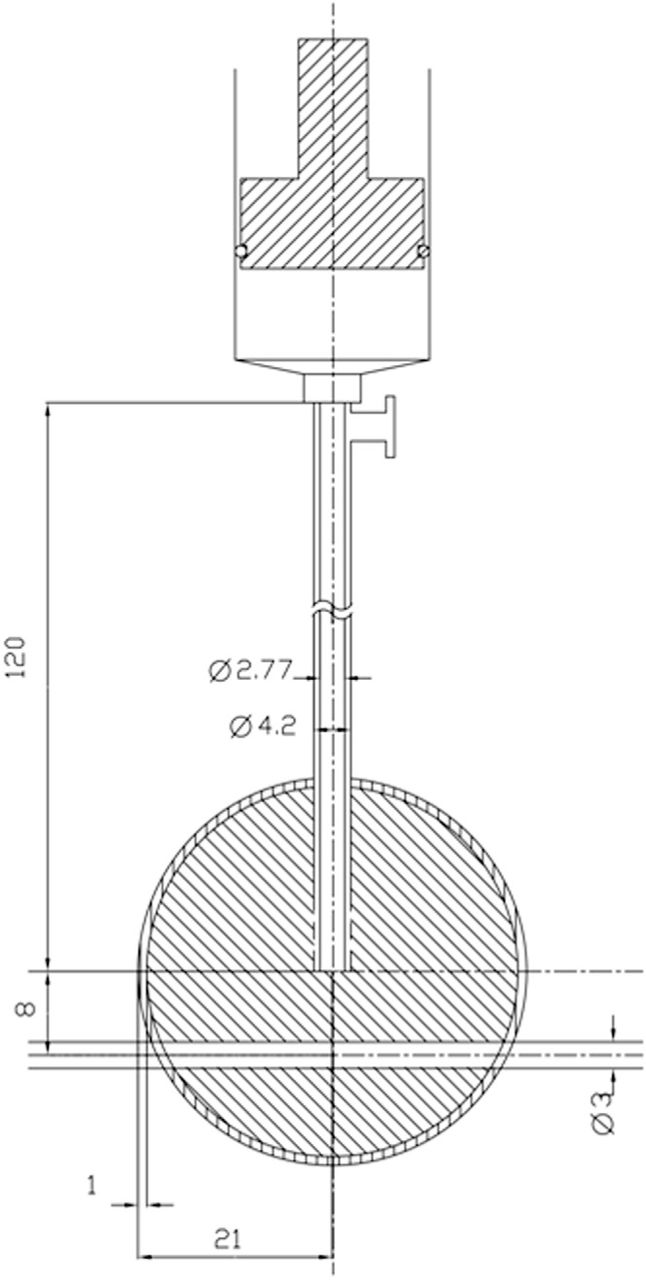
For the delivery of the cement, a novel double-conduit cannula was used to measure the intravertebral pressure while delivering the cement. The novel cannula was formed using double concentric tubing. An internal conduit of 12 G and of 120-mm length with a straight cut tip was used for the delivery of the cement. An outer 8 G tube formed an annular outer space for the IV pressure measurements through a perforated distal end with 8 holes of 1-mm diameter each. The holes were equally spaced on the circumference of the outer tube. A schematic of the experimental setup is shown in Fig. 1.

Schematic drawing of the experimental setup showing the doubleconduit cannula, proximal port for pressure measurement, vertebra model, and the leakage path of 3-mm diameter.
A 5psi pressure sensor was attached to the side port in of the double-conduit needle that is connected only to the annular space. The intravertebral pressure was accordingly sensed through the outer cannula holes and the annular space between the tubes to the pressure sensor (Fig. 1).
The 2 bone cements were mixed according to the specified protocols by the manufacturer. High-viscosity cement was mixed with the aid of the provided mixer with such system for 1 minute, then transferred to the 11cc syringe provided with the system. For low-viscosity, the mixing was done for 2.5 minutes by using the system mixer.
After mixing the cement in both cases, the needles were attached to both systems and injection was applied till bleeding to prime the needles. The needles, which were already marked with an insertion distance 21 mm starting from the distal needle tip, were then inserted in the leakage model injection. The 21-mm mark was used to ensure that the needles were inserted an equal distance into the model. The assembly of the leakage model, with the needle already attached to the delivery system, was then mounted onto a vice. The timing of delivery was coordinated with a stopwatch.
The 11cc cement reservoir of the high-viscosity system supplied 2 successive 5cc injections. The first injection (Group C-a) was performed 3.5 minutes after starting mixing. The second injection (Group C-b) was done 6.5 minutes from starting the mixing process, with 3 minutes as interval between the 2 groups. The high-viscosity 2 successive injections procedure was repeated 5 times.
For the low-viscosity system, the reservoir capacity was sufficient for 3 successive injections of 5cc each. The first injection (Group V-a) was done 3.5 minutes after starting mixing; the second injection (Group V-b) was done 6.5 minutes after stating mixing process; and the third injection (Group V-c) was performed 9.5 minutes after stating mixing process with a 3-minute time interval between injections. The low-viscosity 3 successive injections procedure was repeated 7 times each.
The cement was delivered at approximately 5cc/min. Accurate delivery speed was difficult due to the manual nature of the cement delivery systems. For the high-viscosity system, a half-turn of the hydraulic pump handle was applied approximately every 1.5 second, resulting in 40 half turns per minute, which is equal to 5cc. For the low-viscosity system, a half stroke was delivered every 3 seconds to complete 20 half strokes in a minute, which represents a rate of 5cc injection per minute.
Once the cement delivery started, cement leakage and timing outside of the leakage model was visually inspected. The leaked cement was collected, weighed, and recorded.
To examine the cement filling pattern, each specimen was cut, normal to the specimen axis, into halves, using a water-cooled diamond saw. The cement was colored to enhance the cement filling contrast in the leakage model. Each half was photographed with a digital camera and analyzed with a Matlab code (The Mathlabs, Natick, MA) using the image processing toolbox. The uniformity of the filling was quantified by determining the eccentricity and center point.
Center point shift is used to assess the efficiency of injection starting time in directing the flow. Normally, the filling pattern center point is located lower the horizontal line (X) passing through the injection point (Fig. 1). The effect of changing the injection time start on the center point shift will be addressed. The center point shift (d) in mm is defined as:
The eccentricity (e) of the filled configuration is defined as the eccentricity of an ellipse having the same polar second moment of area as the filled configuration. (It is a measure of how much the profile is flattened.) The more uniform the filled pattern the less the eccentricity; for example, for a straight line the eccentricity is 1, and for a sphere it is 0.
The intravertebral pressure data were gathered for each injection. The temperature and humidity were recorded in each run as well. The results are analyzed using a single factor ANOVA, using confidence bounds approach for the variance analysis.
Results
The study resulted in 5 experimental groups, out of which are 2 for the high-viscosity system (C-a and C-b) and 3 for the low-viscosity system (V-a, V-b and V-c), respectively.
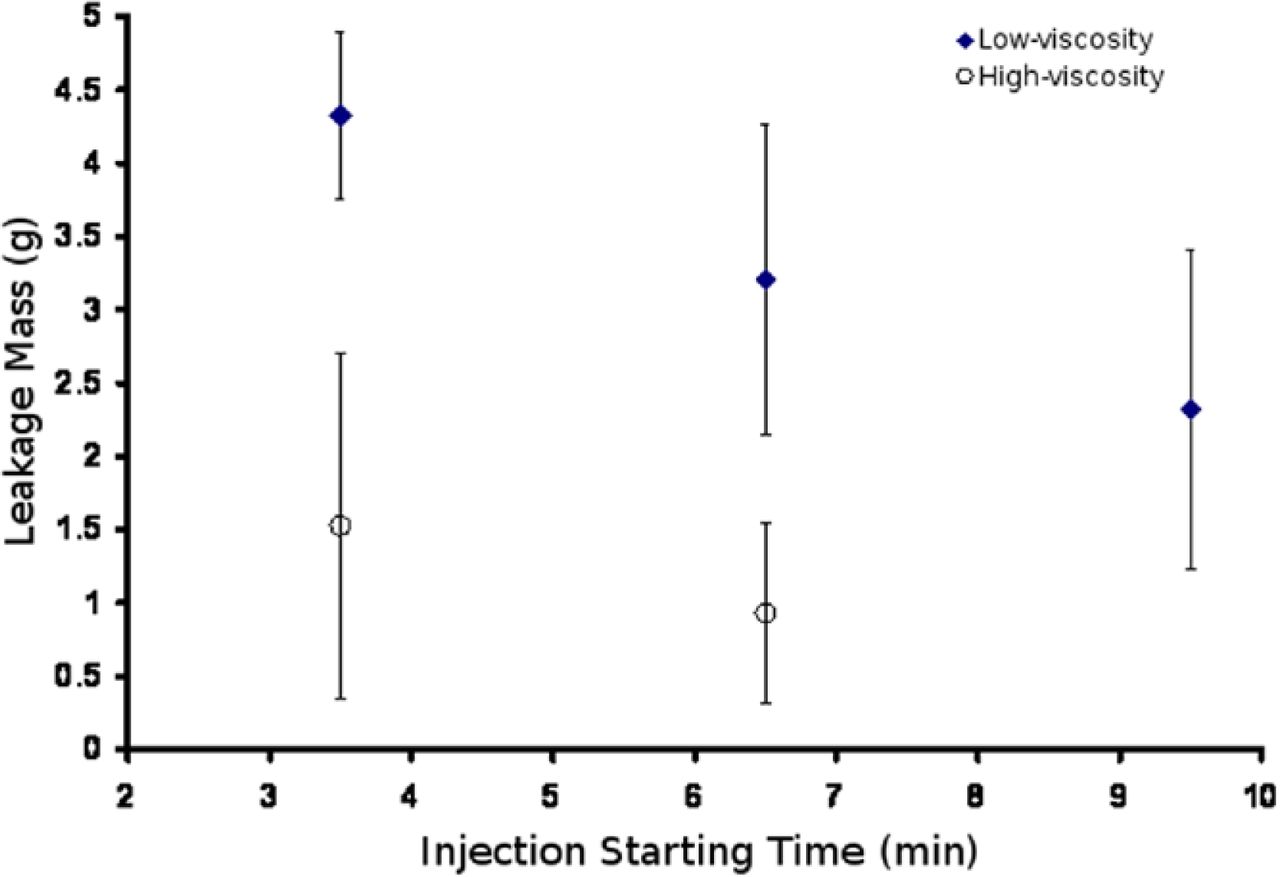
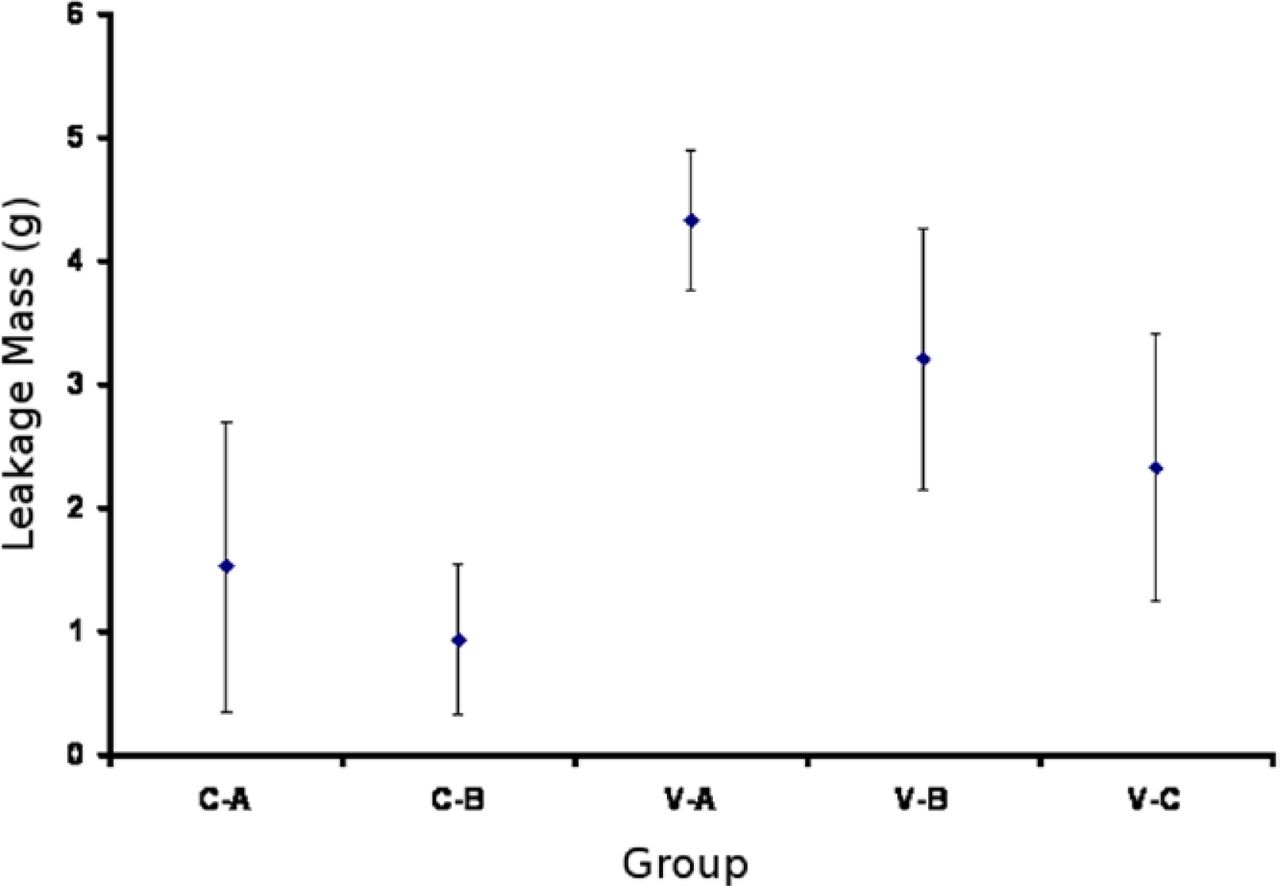
Figure 2 shows the cement leakage mass of the 5 experimental groups with respect to time. Figure 3 shows the same results with respect to each group. In it, the delay in the cement delivery reduced the mass of leaked cement significantly. The high-viscosity groups showed significantly less leakage than the low-viscosity groups. The specific results are listed in Table 1. The leakage mass observed for the high-viscosity group C-a was 1.52 ± 1.17g and that of the low-viscosity group V-a was 4.32 ± 0.57g. This indicates the significant effect (P = .0014). Likewise, for group C-b, using the high-viscosity cement reduces the leakage mass significantly (P = .003). Furthermore, the lowest leakage mass of 0.03g was observed for the highviscosity groups injected at 6.5 minutes. In the case of the low-viscosity system, the lowest leakage mass was 1.35g for the group delivered at 9.5 minutes. There was a pronounced effect of the waiting time on the leakage mass in the low-viscosity groups, as shown in Table 1 (P = .0032). The longer the waiting time, the less leakage in the lowviscosity groups. This trend was not the observed with the high-viscosity groups, which showed insignificant effect of the waiting time on the leakage (P = .3436).
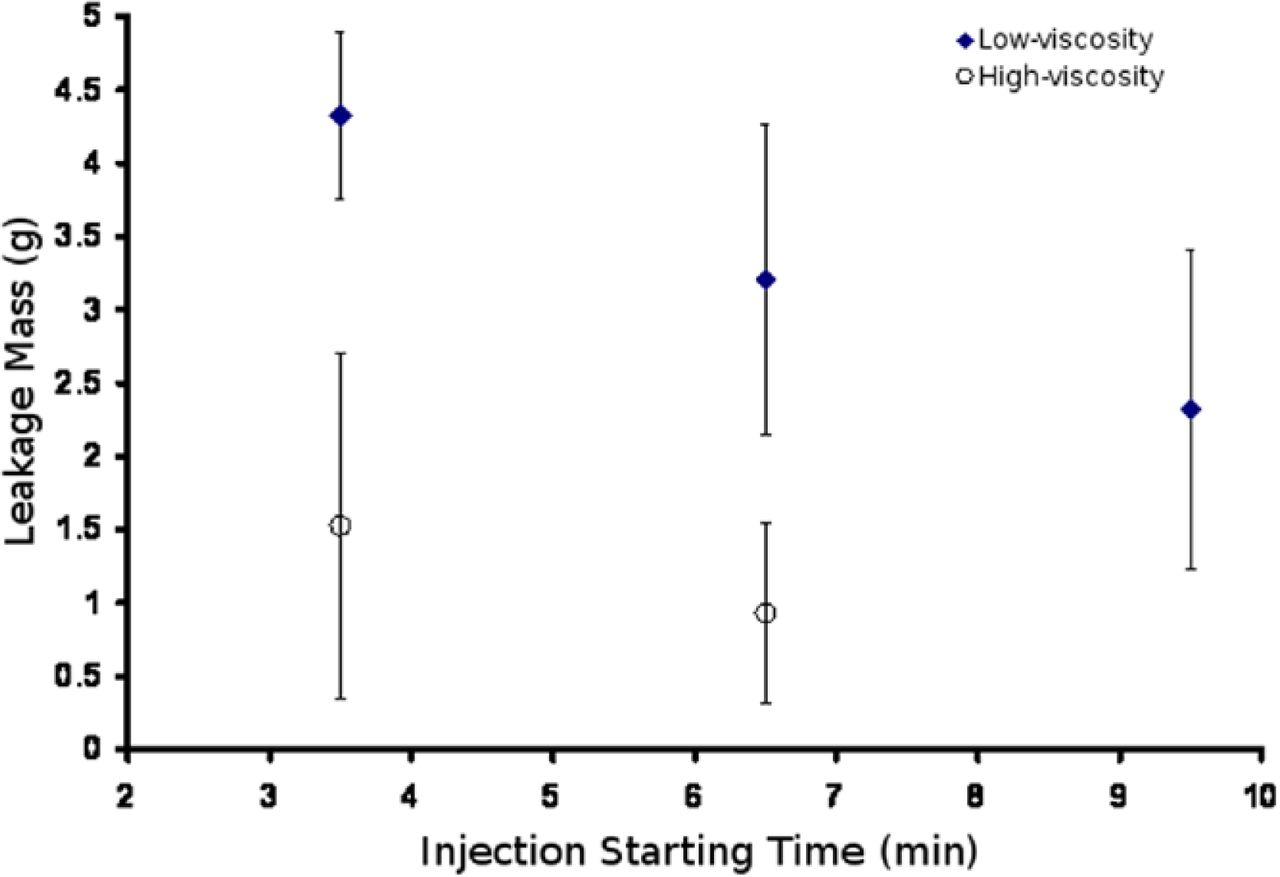
The leakage mass measured for the different systems examined; high-viscosity (C) and low-viscosity (V) regarding to the injection time after starting the mixing.
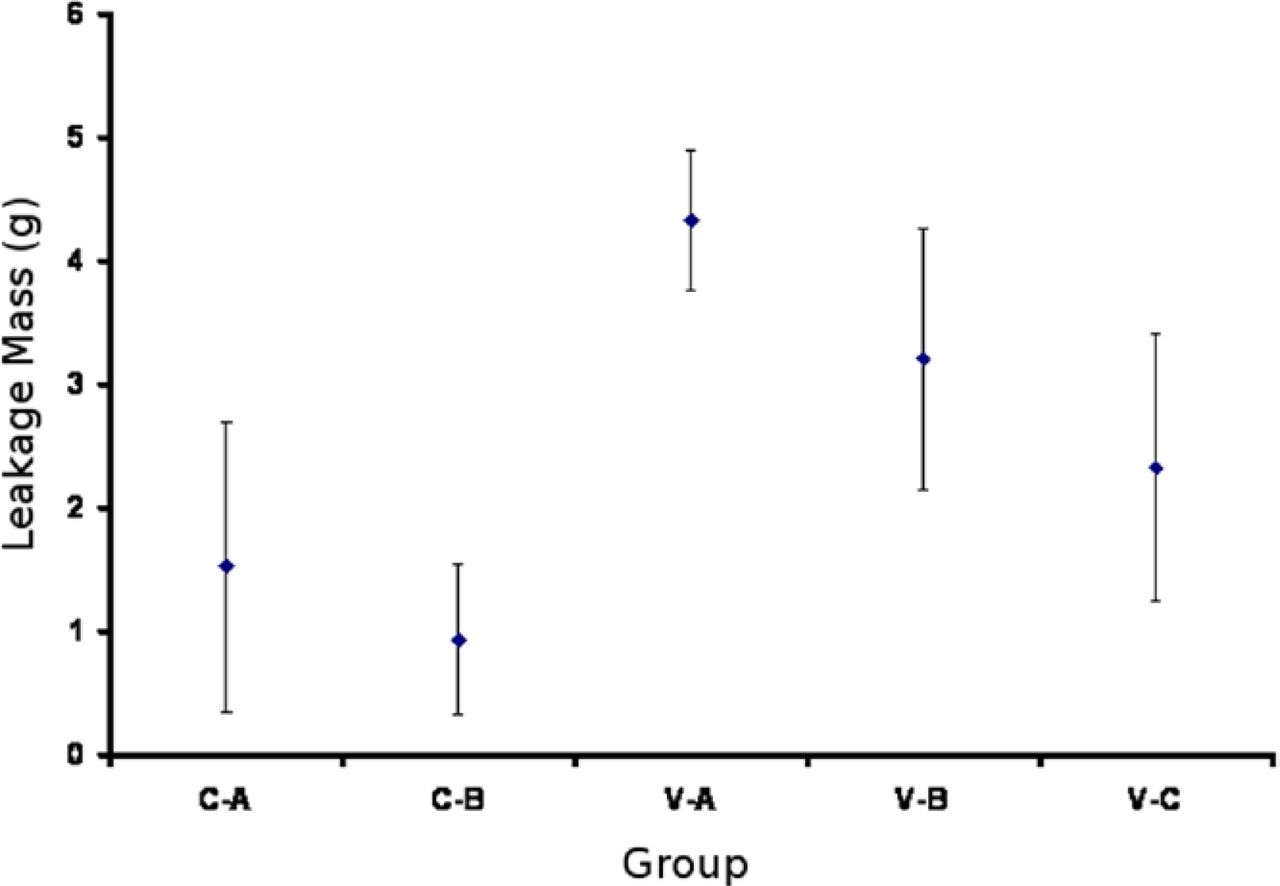
The leakage mass measured for the different systems examined; The 1st letter in the group's name (C) high-viscosity and (V) low-viscosity. the 2nd letter A, B, and C represent the groups regarding to their injection time. (A: 3.5 minutes; B: 6.5 minutes; C: 9.5 minutes after starting the mixing.)
Summary of the eccentricity, center point shift of the filling pattern, and the leakage mass for all the samples tested
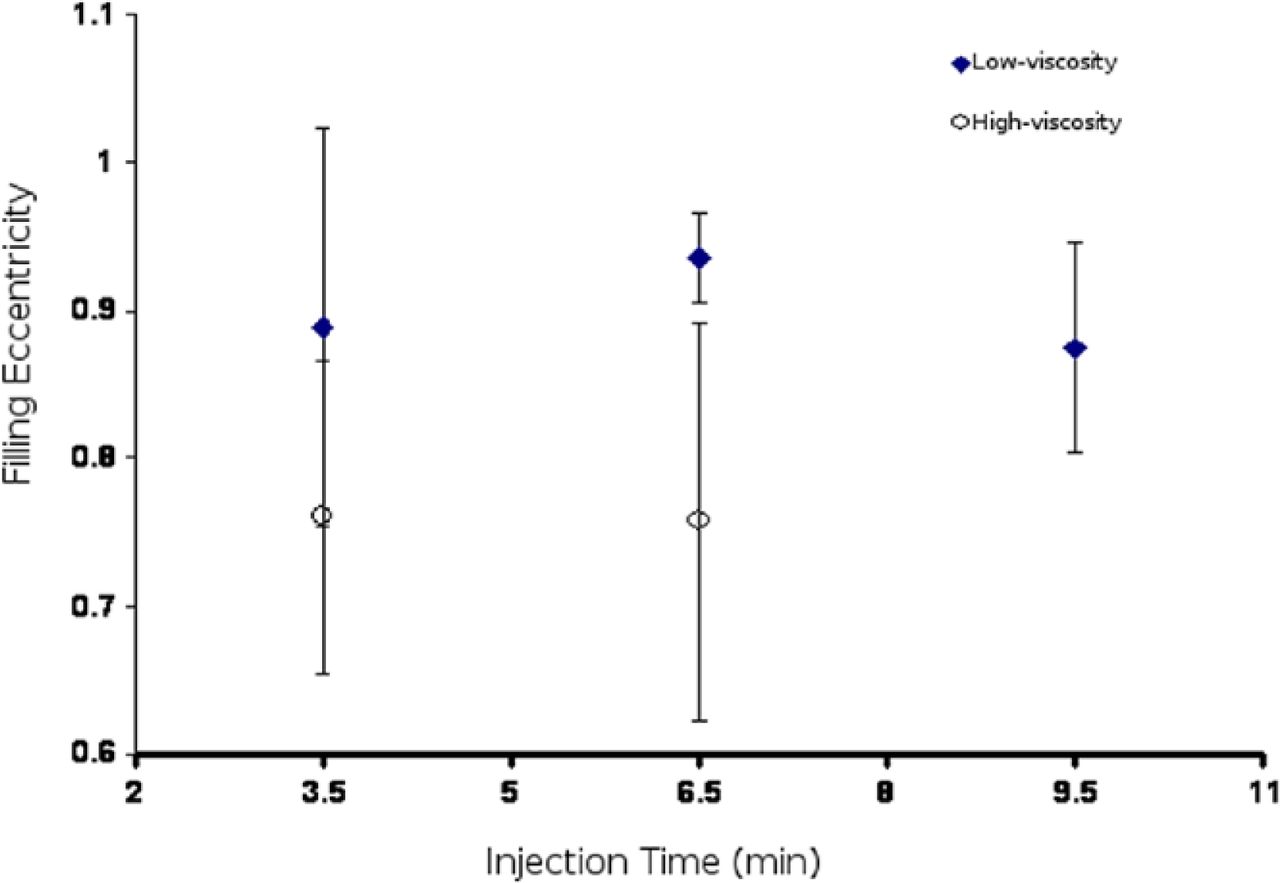
For the filling uniformity, the eccentricity of the filling was measured for all experimental groups, and is depicted in Fig. 4. Figure 5 shows representative examples of the cement filling patterns in all groups. The high-viscosity groups showed significantly higher filling uniformity compared to the low-viscosity groups. However, the change within each group was not significant. For example, there were no significant differences between the 2 groups of the high-viscosity systems as the ANOVA showed (F = 0.88227, P = .43099). Additional details are shown in Fig. 4 and Table 1.
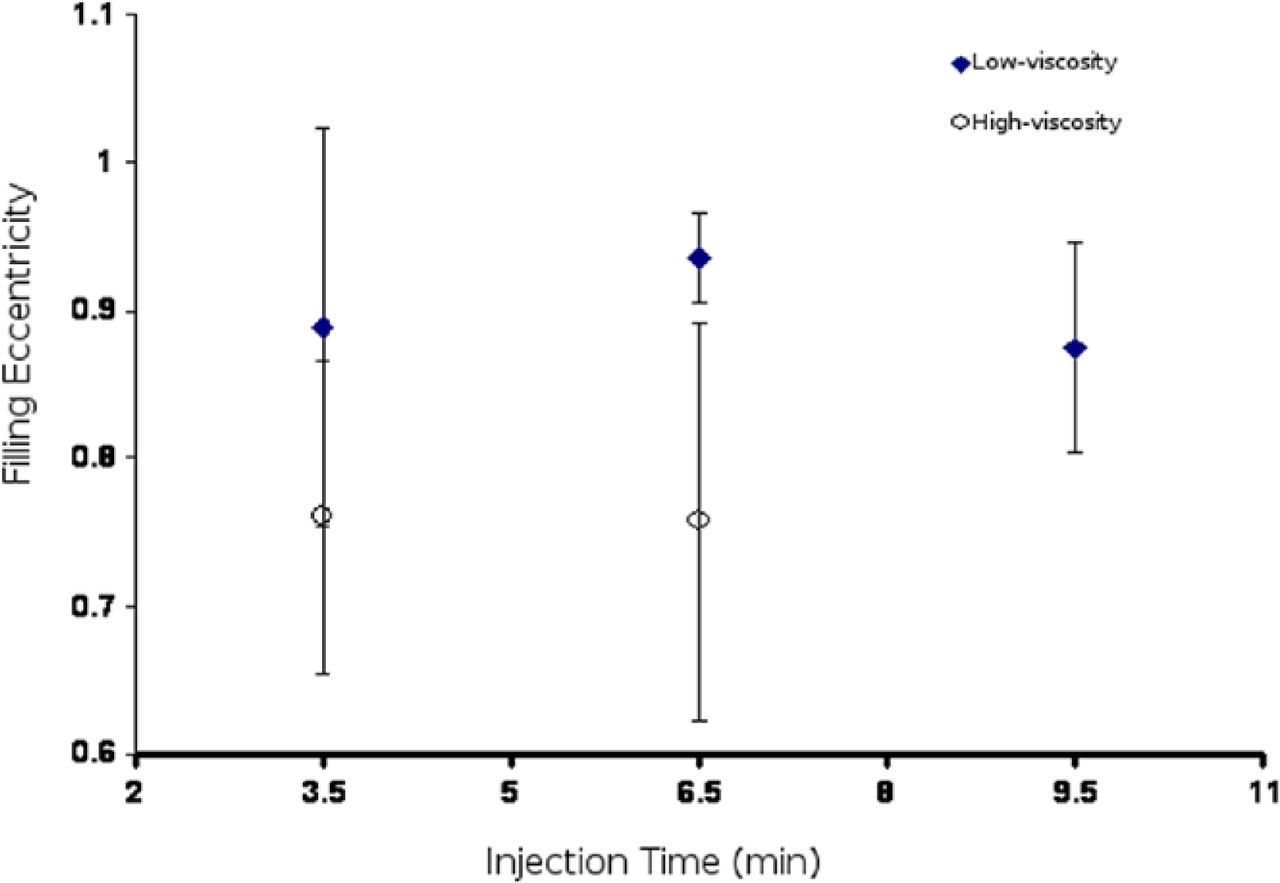
The effect of using Confidence or Vertebroplastic systems injected at different levels on the eccentricity of the filling pattern.

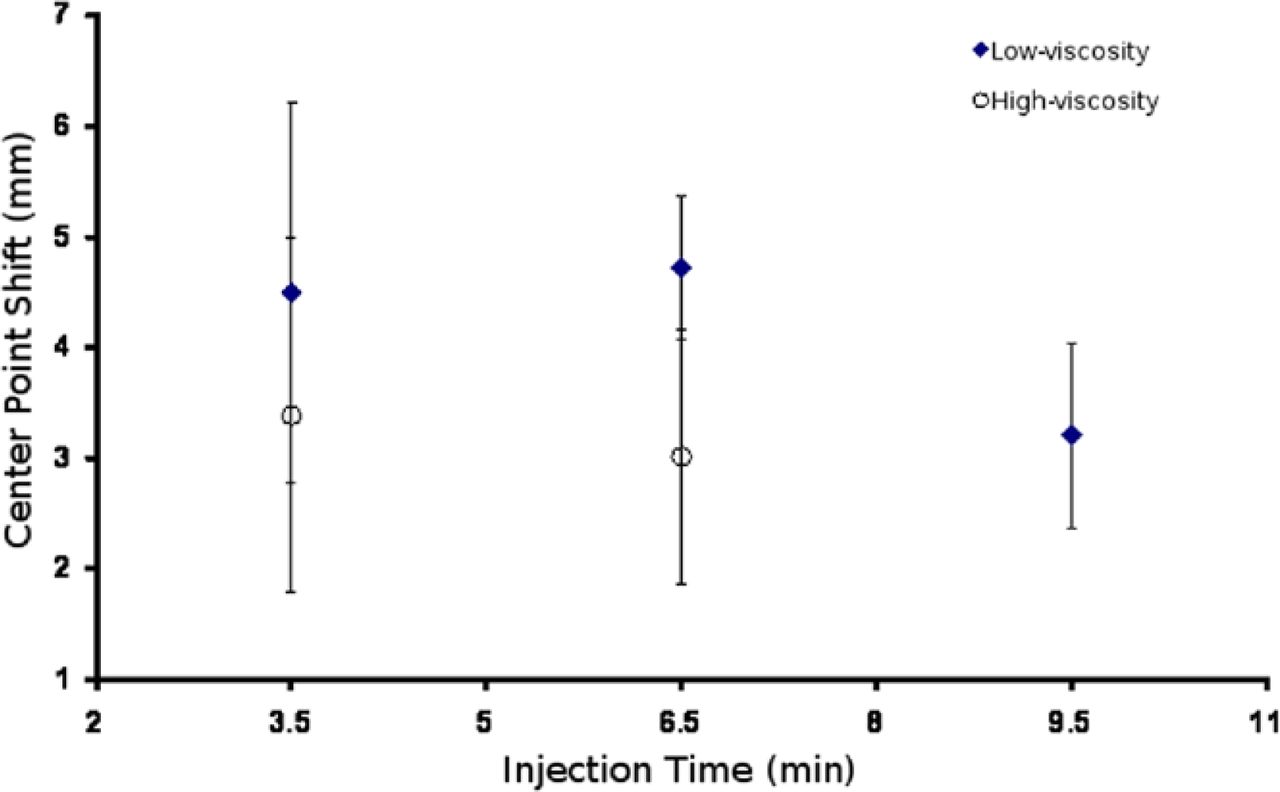
The effect of using high- or low-viscosity systems injected at different levels on the center point shift of the filled pattern.
The second estimate for the uniformity of the filling was performed using the center point shift. The injected samples with high-viscosity cement show much lower shift gain than that of the low-viscosity groups (Fig. 6). For instance, the high-viscosity cement filling after 6.5 minutes has a (3.01 ± 1.15 mm) shift gain; on the other hand, the corresponding low-viscosity cement filling has a (4.72 ± 0.64 mm) shift gain.

The bars represent the filling patterns of the high and low viscosity cements after waiting 3.5 minutes; 6.5 minutes; and after 9.5 minutes.
Figure 5 shows some of the samples which represent the filling pattern of the injected cement. The injection time had no significant effect on the filling pattern of the high-viscosity cement (P = .6848); however the effect of the injection time is more pronounced in the low-viscosity case (P = .0529).
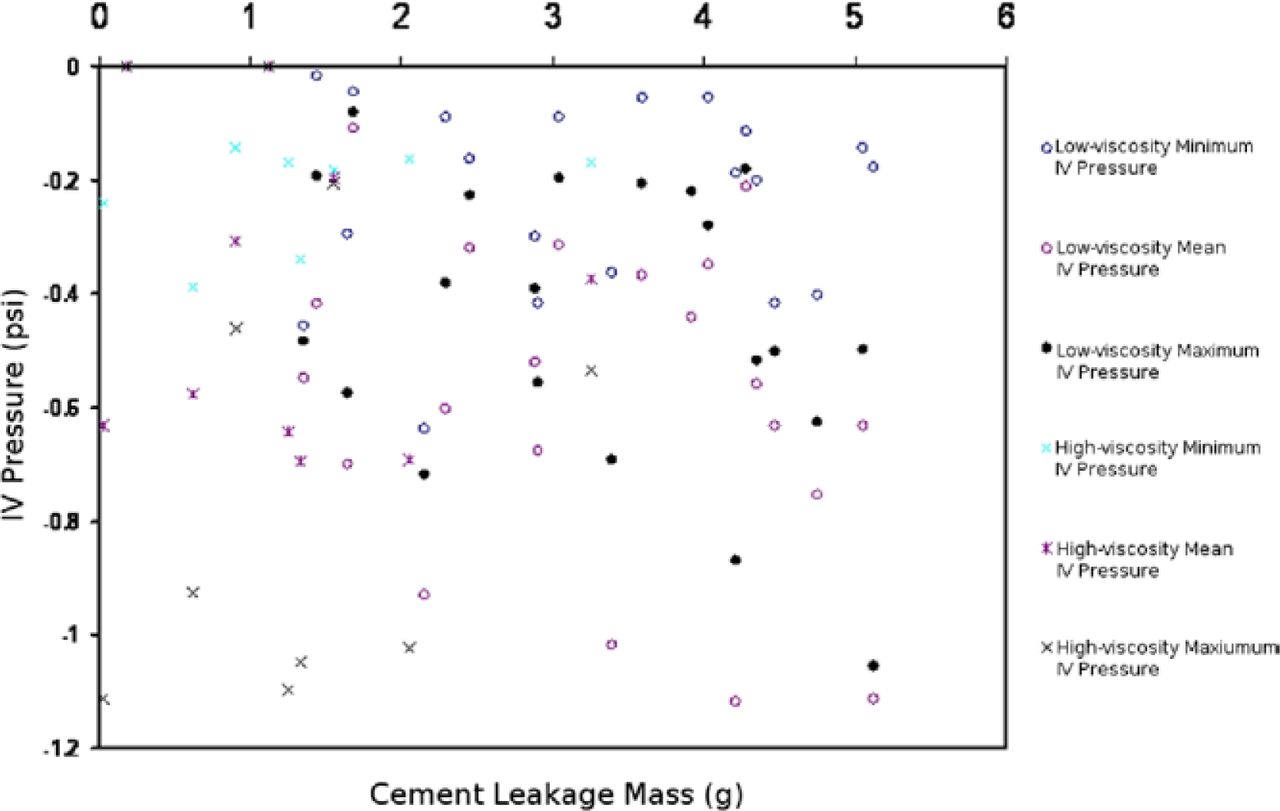
The intravertebral pressure measurements showed no significance with respect to the 5 groups (Figs. 7 and 8). The minimum intravertebral pressure was −0.39psi and the maximum was −0.65psi (F = 0.44, P = .65) in the case of the low-viscosity system, and the minimum IV pressure −0.16psi, and the maximum IV pressure −0.82psi (F = 0.02, P = .89) in the case of the high-viscosity system (Table 2).
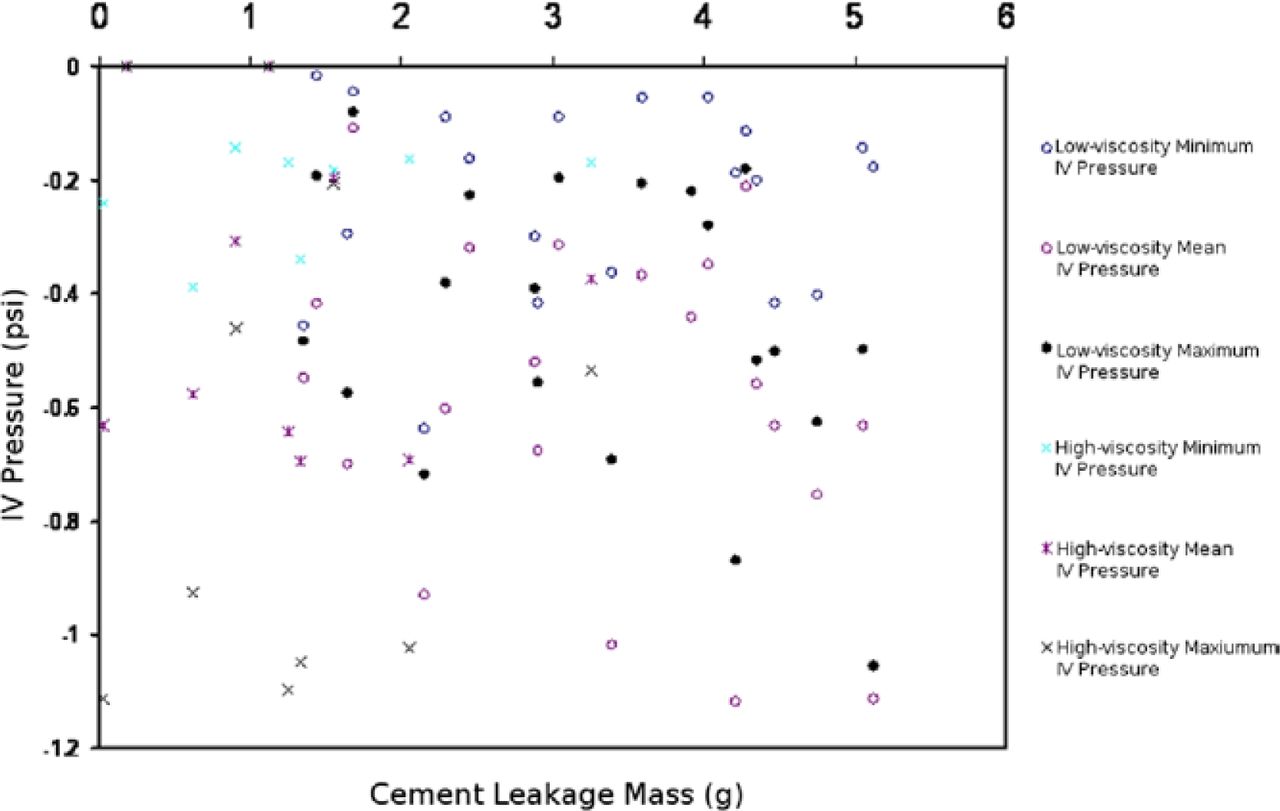
The variation of the intravertebral pressure with the cement leakage mass for the 2 systems used (C and V).

The variation of the intravertebral pressure with the cement leakage mass for the 2 systems used (C and V).
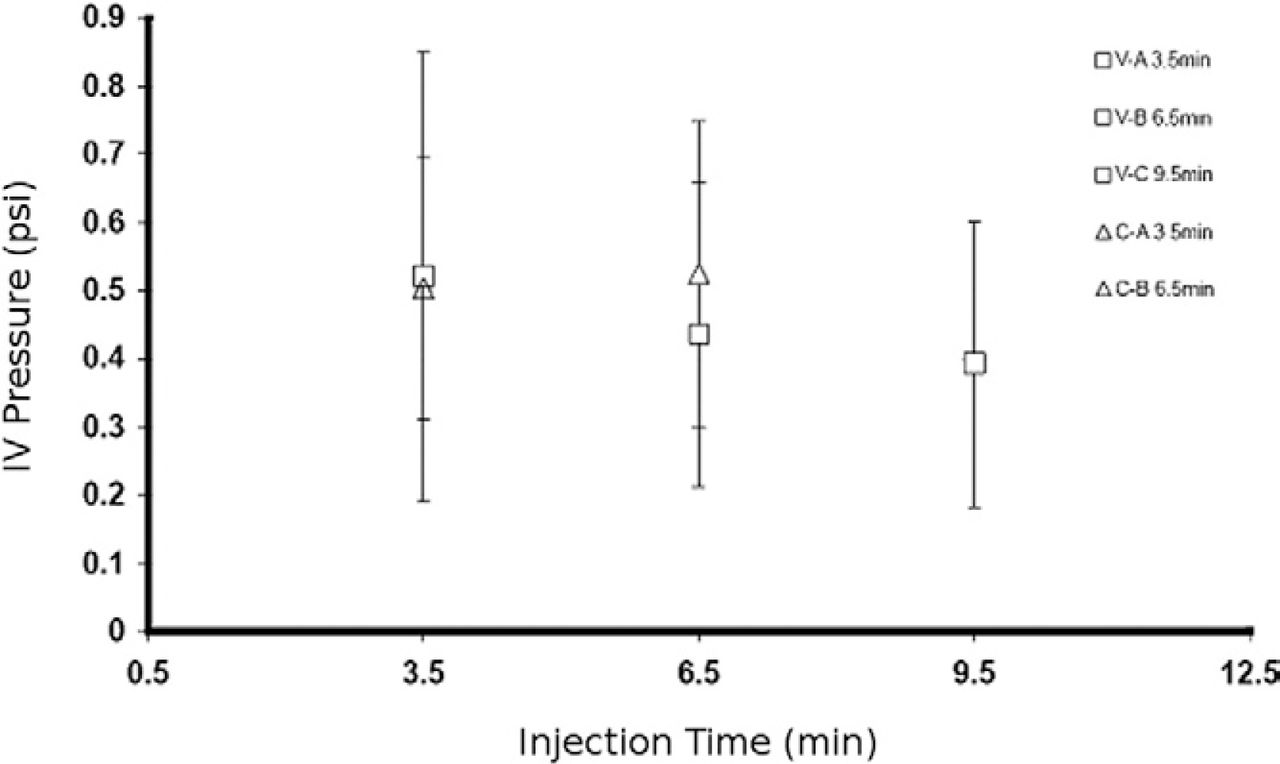
The variation of intra-vertebral pressure (IV) with the injection time
The number of stroke and turns till leakage were counted for the low-viscosity and the high-viscosity cements, respectively. The numbers of stroke or turns till leakage were increased with delaying of starting the injection in most of the cases (Table 1).
Discussion
The study compared the leakage, filling, and intravertebral pressure behavior of the high-viscosity and low-viscosity cement delivery systems based on a laboratory leakage model established by Baroud et al.3 The importance of uniform cement filling and reduced cement leakage is evident for vertebral body augmentation procedures.
The results of the study show significant superior results for the high-viscosity system; specifically, the filling uniformity increased and the cement leakage reduced in all high-viscosity groups compared to the low-viscosity groups.
Interestingly, there seems to be no relationship between the intravertebral pressure values and the cement leakage or filling patterns. Also, there was no significant increase in intravertebral pressure when the cement was delivered at a later point of time. For example, when low-viscosity cement was injected at 9.5 minutes compared to 3.5 minutes, the pressure measurement did not increase significantly. Likewise, there have been no significant differences between the low-viscosity and high-viscosity groups. These results are not surprising given the fact that the intravertebral pressure is mainly determined by the flow rate and viscosity of the displaced marrow, and not displacing cement.9
It should be noted that this study has a number of limitations. The most important one is that it is based on a laboratory model made of aluminium. Though the general trend of cement leakage and filling is not affected by the nature of the trabecular structure of the model, some limitations may apply to the ability of thick cement to penetrate the trabecular bone structure in clinical setting, as compared to pushing the osteoporotic bone away and thus creating a larger bone cavity. This model is not in a position to address this question. However, for the physician performing vertebroplasty, it is important to be aware of the quality of the bone being treated and, therefore, choose the adequate thickness of the cement to avoid destroying the trabecular bone structure.
Extended references
Cement leakage during vertebroplasty can be predicted on preoperative MRI.
Hiwatashi A, Ohgiya Y, Kakimoto N, et al.
OBJECTIVE: Previous studies have shown that cement leakage into an adjacent disk space is a risk factor for new fracture after vertebroplasty. The purpose of this study was to investigate the use of preoperative MRI for predicting such cement leakage. MATERIALS AND METHODS: Our institutional review board approved this retrospective study and waived the requirement of informed consent. We studied preoperative MRI of 46 vertebroplasty patients (107 vertebral bodies). Endplate cortical defect, abnormal T2 hyperintensity in adjacent disk space, intravertebral cleft, degree of compression, and wedge angle were correlated to the incidence of cement leakage into the adjacent disk. Patient age, sex, and location of treated vertebral body were also evaluated. We used logistic regression analysis and Fisher's exact probability test to analyze the association between cement leakage and these observations. RESULTS: Cortical defect in the endplate of the treated vertebral body, abnormal T2 hyperintensity in the adjacent intervertebral disk, and absence of intravertebral cleft were associated with cement leakage into the disk space (P < 0.05). There was no statistically significant association between cement leakage into the disk and degree of compression, wedge angle, location of treated vertebral body, patient age, or sex (P > 0.05). CONCLUSION: Cement leakage into an adjacent disk is more common when there is a cortical defect in the endplate and increased T2 signal in the adjacent disk and is less common if there is an intravertebral cleft.
High-viscosity cement significantly enhances uniformity of cement filling in vertebroplasty: an experimental model and study on cement leakage.
Baroud G, Crookshank M, Bohner M.
STUDY DESIGN: Experimental study using a laboratory leakage model. OBJECTIVE: To examine the working hypothesis that high-viscosity cements will spread uniformly, thus significantly reducing the risk of leakage. SUMMARY OF BACKGROUND DATA: In vertebroplasty, forces that govern the flow of bone cement in the trabecular bone skeleton are an essential determinant of the uniformity of cement filling. Extraosseous cement leakage has been reported to be a major complication of this procedure. Leakage occurs due to the presence of a path of least resistance caused by irregularities in the trabecular bone or shell structure. Ideally, cement uniformly infiltrates the trabecular bone skeleton and does not favor specific paths. Cement viscosity is believed to affect the infiltration forces and flow during the procedure. Clinically, altering the time between cement mixing and delivery modifies the viscosity of bone cement. METHODS: An experimental model of the leakage phenomenon of vertebroplasty was developed. A path, simulating a blood vessel, was created in the model to perturb the forces underlying cement flow and to favor leakage. Cement of varying viscosities was injected in the model, and, thereafter, the filling pattern, cement mass that has leaked, time at which leakage occurred, and injection pressure were measured. RESULTS: A strong relationship was found between the uniformity of the filling pattern and the elapsed time from cement mixing and viscosity, respectively. Specifically, 3 distinct cement leakage patterns were observed: immediate leakage was observed when cement was injected 5-7 minutes following mixing. The cement was of a low viscosity and more than 50% of the total cement injected leaked. Moderate leakage was observed when injection occurred 7-10 minutes following mixing. Less than 10% of the cement leaked, and the viscosity was at a transient state between the low viscosity of immediate leakage and a higher viscosity, doughy cement. Cement leakage ceased completely when cement was delivered after 10 minutes. The viscosity of the cement in this case was high, and the cement was of a dough-like consistency. CONCLUSIONS: High-viscosity cement seems to stabilize cement flow. However, the forces required for the delivery of high-viscosity cement may approach or exceed the human physical limit of injection forces. Although the working time of the cement is about 17 minutes, it may not be manually injectable with a standard syringe and cannula after 10 minutes, at which time cement leakage ceased completely.
Theoretical and experimental model to describe the injection of a polymethyl methacrylate cement into a porous structure.
Bohner M, Gaser G, Baroud G, et al.
A theoretical approach was used to determine the distribution of a poly(methylmethacrylate) cement after its injection into a porous structure. The predictions of the model were then compared to experimental results obtained by injecting a polymethylmethacrylate cement into an open-porous ceramic filter. The goal was to define a model that could predict what factors affect the risk of cement extravasation and hence how the risk of cement extravasation can be minimized. The calculations were based on two important rheological laws: the law of Hagen-Poiseuille and the law of Darcy. The law of Hagen-Poiseuille describes the flow of a fluid in a cylindrical tube. The law of Darcy describes the flow of a fluid through a porous media. The model predicted that the extravasation risk was decreased when the cement viscosity, the bone pore size, the bone permeability and the bone porosity were increased, and when the diameter of the extravasation path and the viscosity of the marrow were decreased. Experimentally, the effect of the marrow viscosity and extravasation path could be evidenced. Therefore, the model was believed to be an adequate approximation of the experimental behavior. In conclusion, the experimental results demonstrated that the model was adequate and that the best practical way to decrease the risk of extravasation is to increase the cement viscosity.
Experimental and theoretical investigation of directional permeability of human vertebral cancellous bone for cement infiltration.
Baroud G, Falk R, Crookshank M, et al.
The use of acrylic polymers in infiltrating the porous bone structure is an emerging procedure for the augmentation of osteoporotic vertebrae. Although this procedure is employed frequently, it is performed based on empirical knowledge, and therefore, does not take into consideration the porosity-dependent permeability of human vertebral cancellous bone. The purpose of this study was to: (a). experimentally and theoretically investigate interdependence of the vertebral cancellous bone permeability and porosity, and (b). examine if the bone permeability of spinal cancellous bone can be predicted using bone mineral density measurements. If these relations can be established, they can be useful in optimizing the injection conditions for predicable cement infiltration. To determine the porositydependent and directional permeability, 34 bone cores-20 samples in the superior-inferior (SI) direction and 14 in the anterior-posterior (AP) direction-were cut from 20 lumbar vertebrae and infiltrated with silicone oil with a viscosity matching that of PMMA. The permeability of the cores was determined based on Darcy's law. The mean permeability of SI and AP cores was 4.45+/− 1.72 × 10(−8) and 3.44+/− 1.26 × 10(−8)m(2), respectively. An interesting finding of this study was that the permeability of the AP cores was approximately 78% of that of SI cores, though the porosity of the SI and AP cores taken from the same vertebra was approximately equal. In addition, we provided a theoretical model for the porosity-dependent permeability that accurately described non-linear dependency of the bone permeability and porosity in both directions. Although the relation of the bone permeability and porosity was established, bone mineral density was a weak predictor of the bone permeability. The experimental and theoretical results of this study can be used to understand polymer flow in cement infiltration procedures.
Footnotes
This research work was partially supported by a research grant from DePuy Spine.
- © 2010 SAS - The International Society for the Advancement of Spine Surgery. Published by Elsevier Inc. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Dr. Hassan Serhan and C. Marchek are employees of DePuy Spine.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.