


Abstract
Study design Retrospective cohort from randomized prospective clinical trial.
Objective Evaluate incidence of dysphagia between instrumented ACDF and a no-profile cervical disc arthroplasty.
Summary of background data Dysphagia is a well-known complication following anterior cervical discectomy and fusion (ACDF) and the etiology is multifactorial. One potential source for postoperative dysphagia involves the anterior profile of the implant used. Hence, a no-profile cervical disc arthroplasty could theoretically have fewer soft tissue adhesions and a lower incidence of dysphagia. The purpose of this study is to compare the incidence of dysphagia at least 1 year postoperatively following ACDF with anterior plating and a no-profile cervical disc arthroplasty.
Methods A cohort of 87 patients meeting the inclusion criteria for the prospective, randomized, multicenter IDE trial of ProDisc-C versus ACDF were evaluated for dysphagia. Forty-five patients were randomized to receive cervical arthroplasty and 42 patients were randomized to the ACDF and plate group. The Bazaz-Yoo dysphagia questionnaire was administered in a blinded fashion after completion of at least 12 months follow-up.
Results Follow-up averaged 18.2 months and included 76 (87%) of the 87 enrolled, with 38 of the original 45 in the arthroplasty group and 38 of the original 42 in the ACDF group. Six of 38 (15.8%) in the arthroplasty group versus 16 of 38 (42.1%) in the ACDF group reported ongoing dysphagia complaints. This was found to be statistically significant (P = .03).
Conclusion This study suggests a significantly lower rate of dysphagia with a no-profile cervical disc arthroplasty compared to instrumented ACDF for single level disc disease between C3-7. Though there are many potential etiologies, we hypothesize this is related to the lack of anterior hardware in the retropharyngeal space. Operative technique, operating time, and significant midline retraction did not seem to result in more dysphagia complaints. Future studies comparing cervical disc arthroplasty and no-profile fusion devices may help delineate the effect that anterior instrumentation profile has on postoperative dysphagia.
The treatment of cervical radiculopathy and myelopathy with anterior cervical discectomy and fusion (ACDF) has proven to provide good clinical results and high patient satisfaction scores.1, 2 However, postoperative dysphagia is a well-known complication, with incidence ranging widely in various reported series.3–5 The etiology of dysphagia is multifactorial, and has been attributed to hematoma, pharyngeal plexus denervation, vocal cord paralysis, adhesion formation, plate profile, and swelling due to biologic agents.3, 5–8 Recent studies evaluating plate design suggest a lower, smoother anterior profile may correlate with reduced incidence of dysphagia following ACDF.7, 9 Other studies have demonstrated improvement of dysphagia with removal of the anterior cervical plates and release of mechanical adhesions of the esophagus.10 With this in mind, the advent of new technologies with no anterior profile such as cervical disc arthroplasty and stand-alone plate-spacer constructs could potentially offer the benefit of decreased incidence of dysphagia compared to ACDF with anterior plating.
The purpose of this study is to compare the incidence of dysphagia after instrumented ACDF versus a no-profile arthroplasty for a single disc. With evidence that anterior profile and plate adhesions to esophagus strongly correlate with increased dysphagia, we hypothesize that the arthroplasty group will have a lower incidence of dysphagia at 1 year. This could be due in part to the absence of an anterior profile, preservation of paroxysmal motion limiting adhesions, or a combination thereof. However, if factors such as esophageal retraction common to the operative technique of both procedures show a strong correlation with dysphagia, the null hypothesis may hold true in that there is no clinical difference between dysphagia after instrumented ACDF verses a no-profile cervical arthroplasty.
Materials and methods
Our study population consists of a cohort of patients enrolled in the prospective, randomized multicenter IDE trial of ProDisc-C (Synthes, West Chester, Pennsylvania) versus ACDF. Included in the study were patients treated for single level disc disease between C3-7, randomized to ACDF and cervical arthroplasty. Two of the 14 centers performed an independent questionnaire outside of the FDA protocol to investigate the rates of dysphagia in both groups. Institutional Review Board permission was granted to review the postoperative data. This retrospective data was based on telephone interviews after completion of their 1-year follow-up exam. We used the Bazaz-Yoo dysphagia questionnaire administered in a blinded fashion.3 Our study included 45 patients in the arthroplasty group and 42 patients in the ACDF group. As part of the FDA IDE trial, demographics and intraoperative data were recorded, as well as adverse events such as dysphagia complaints at follow-up visits. Preoperative counseling regarding dysphagia was indifferent between the 2 groups. In the study arm receiving the questionnaire, the dysphagia score was calculated as follows: 0 represented no dysphagia, 1 represented mild with rare symptoms involving solids only, 2 indicated moderate severity with occasional solid food symptoms and none or rare liquid symptoms, and 3 indicated severe dysphagia with frequent symptoms including the majority of solid food (Table 1).3 The frequency and intensity of symptoms were recorded and compared. Statistical difference between ACDF and arthroplasty were determined using a Chi-square analysis for dysphagia categories, Fisher's Exact test for comparing the incidence of some degree of ongoing dysphagia, and a Mann-Whitney U test was used for the total dysphagia score. The significance level was established at .05 for all statistical tests. A sample size calculation for the dysphagia outcome was performed using a 1-sided superiority test for comparing 2 binomial populations. Using a type I error of 5% and assuming a treatment group difference (ie, delta) of 25%, 45 patients per group are required in order to achieve 80% power.
Bazaz-Yoo grading dcore
Results
Patient demographic data included gender, age, body mass index, litigation status, smoking, and employment status. There were no statistically significant differences between the 2 groups with regard to the above demographics (Table 2). As expected, the C5-6 level was the most common index level, followed by C6-7 (Table 3). The mean operative time showed statistical significance with arthroplasty averaging 89.4 minutes and ACDF averaging 81.3 minutes (P = .0159). Average blood loss was also found to be statistically significant with arthroplasty averaging 97.7 ml and ACDF 66.5 ml (P = .0029).
Demographics of patients participating in the study
Levels operated
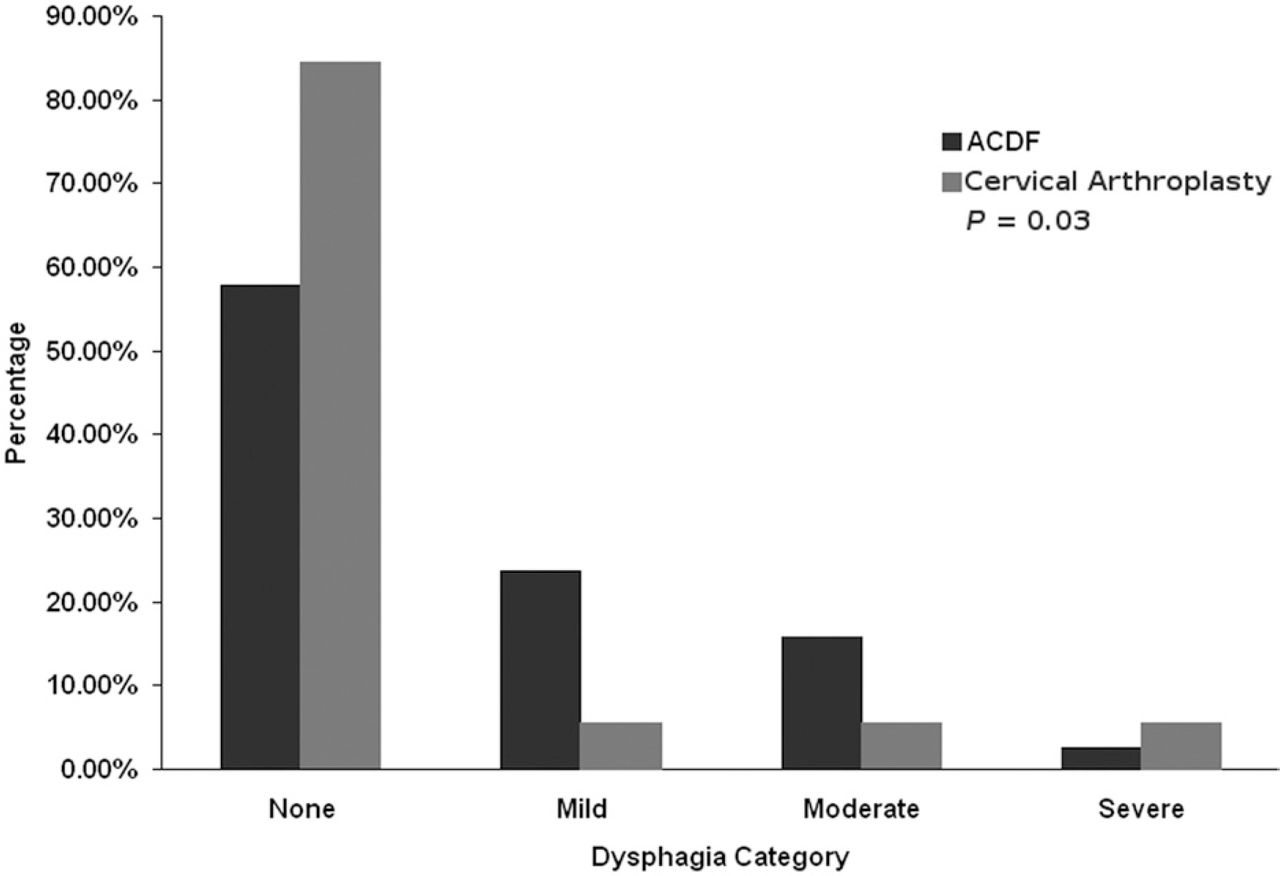
The overall follow-up of patients completing the Bazaz-Yoo questionnaire was 87.4% (76 out of 87). This included 38 of 45 in the ProDisc-C group and 38 of 42 in the ACDF group. The average follow-up was 18.2 months. At 12 months postop, 15.8% (6 out of 38) of arthroplasty patients and 42.1% (16 out of 38) of ACDF patients reported some degree of ongoing dysphagia; this difference in intensity was found to be statistically significant (P = .01; 1-sided Fisher's Exact test). The stratification of the severity of complaints for each group showed the majority of patients had mild to moderate symptoms. In the arthroplasty group, there were 2 patients who rated their dysphagia as mild, 2 as moderate, and 2 as severe. In the ACDF group, the patient dysphagia ratings were 9 mild, 6 moderate, and 1 severe. The distribution of the severity of complaints was also significantly different between groups across dysphagia categories (P = .03; Chi-square test) (Fig. 1).

Rates of dysphagia severity between ACDF and no-profile cervical arthroplasty.
Retrieving the adverse events data reported as part of the FDA IDE clinical trial at the 2 sites included in this study, 1 patient in the arthroplasty group, and 2 in the ACDF group reported symptoms of dysphagia. In our questionnaire assessment, each of these patients rated their dysphagia as moderate or severe. Further investigation showed that 4 of the patients in the ACDF group were determined to have a pseudoarthrosis (9.5%), 2 of which had reported dysphagia. One patient who underwent ACDF reported chronic anterior neck myofascial pain with moderate dysphagia. This patient underwent revision surgery to remove the anterior plate, though the dysphagia did not resolve.
Discussion
This study compares the incidence of dysphagia after ACDF versus a no-profile cervical arthroplasty in similar patients. As a cohort study arm of the prospective, randomized multicenter IDE trial, our patient demographics and indications were well-controlled. The results of our study support the working hypothesis that a no-profile arthroplasty compared to instrumented ACDF demonstrates a statistically significant lower incidence of dysphagia. This held true for overall incidence of dysphagia as well as intensity of the complaints. However, there did not seem to be a significant difference for those reporting severe symptoms. Given that severe dysphagia was a rare event, a much larger study population would likely be needed in order to determine a difference between the 2 treatment groups. Given the differences between the groups in patients having moderate severity dysphagia (2 of 45 arthroplasty versus 9 of 42 ACDF), as well as the intensity of complaints, the authors feel there is both a statistically and clinically significant difference between the treatment groups.
Increased operative times and blood loss were found to be statistically significant with arthroplasty averaging 8.1 minutes longer and 31.2 ml increased blood loss compared to ACDF. However, these values do not seem to be clinically significant and do not appear to result in any increase in dysphagia. Utilizing the same static retractors for both groups helps to control for this variable, and again was thought not to be a clinically significant factor in our study. Though Tortolani has shown in a cadaveric study significantly greater retraction pressures with ACDF compared to cervical arthroplasty using the same dynamic retractors, a recent prospective study questions the correlation between esophageal retraction pressures and postoperative dysphagia. 11, 12 Another recent study supports the theory that dynamic versus static retraction has an effect on postoperative dysphagia.13 If this were a leading factor contributing to postoperative swallowing difficulties, one would expect the rates of postoperative dysphagia to be similar using the same retractors for both arms of the study. This was not the supported by our findings which show increased dysphagia in the ACDF group.
Lee et al demonstrated that lower profile anterior plate design lessens the incidence of dysphagia in patients undergoing anterior cervical fusions.7 However, a recent prospective study questions the role of plate thickness as a cause of dysphagia.14 The cervical plating study sponsored by the Cervical Spine Research Society (CSRS) comparing instrumented and uninstrumented ACDF patients showed a slight increase in the incidence of dysphagia with anterior instrumentation of 7.9% vs. 5.3% in the uninstrumented group at 24 months follow-up.15 Fogel et al reported on the surgical exploration and removal of anterior hardware for persistent moderate to severe dysphagia symptoms.10 Intraoperative findings for all patients demonstrated significant adhesion of the pharynx and esophagus to the plate by scar, which was released before plate removal. Fift-five percent of patients had resolution of their dysphagia and an additional 32% reported improvement to mild symptoms. These studies reinforce that anterior hardware likely has a role in the increased rates of dysphagia beyond the approach related incidence. The results of our study would also support the theory that anterior hardware and its profile play a role in the development of these symptoms.
The lack of hardware anterior to the spine may not be the only factor that leads to the lower rate of dysphagia in these arthroplasty patients. Motion could be a variable that lessens the amount of scar tissue that forms. It may also lead to a more flexible type of scarring that does not interfere with the complex, coordinated pharyngeal movements required for proper swallowing. This assumption is unable to be proven with the current study, but may be topic of future investigations.
The rate of dysphagia complaints with a noninstrumented fusion in the CSRS study are less than the rates in the arthroplasty group in this study.4, 15 The rate is 15.8% demonstrated in this study, compared to 5.3% in the CSRS nonrandomized study.15 Our study compares similarly to the 12.5% rate of dysphagic complaints by Bazaz et al, which was a prospective randomized study. The instrumented fusion dysphagia rate at 1 year of 42.1% was significantly more than these previously mentioned studies. This may be related to the plate profile, operative techniques, or the smaller sample size in this study.
Most dysphagia that occurs improves in the first 6 months and probably results in an overall incidence of all severities of 12.5-35.1% at greater than 1 year.3, 6 This study demonstrates a 42.1% rate of dysphagia in the instrumented ACDF group, which is higher than the rates in more recent prospective studies. This again may be related to the plate profile, operative techniques, or the smaller sample size in this study.
Nonunion and scar formation have been documented causes of dysphagia symptoms in anterior cervical fusion patients. One patient in the ACDF group had the plate removed because of anterior myofascial pain and persistent moderate dysphagia symptoms. This patient did not improve after removal of the plate. Pseudarthrosis was identified in 4 patients, with only 2 reporting dysphagic symptoms. None of the patients had loosening or migration of the implants or graft.
Although the patient demographics and surgical indications were well controlled, as this was a subset of an FDA IDE trial, the study does have limitations. Data collected for this cohort was done in a retrospective manner. Therefore, there was not a baseline preoperative dysphagia score, which is a potential criticism. Despite the study questionnaire being administered in a blinded fashion, the timing of questionnaire in relation to postoperative date was not tracked or matched among the 2 groups. This could influence the data, as dysphagia tends to decrease over time. Additionally, while the Bazaz-Yoo scoring system is an accepted tool for evaluating dysphagia, patient responses are overall subjective. Also, patient age has been associated with increased risk of dysphagia. While it may have been more informative to delineate ages of those who scored positively on the dysphagia questionnaire, the age demographics between the 2 groups was found to be similar. Therefore, only the total number and category of dysphagia complaints were felt to be relevant to our study.
This study suggests a significantly lower rate of dysphagia with no-profile cervical disc arthroplasty compared to instrumented ACDF. We hypothesize that this correlation is related to the lack of anterior hardware in the retropharyngeal space. Continued motion at the operated level may play a small role, but was unable to be evaluated properly with the current study. Operative technique including increased operating time and significant midline retraction required for proper implantation of a cervical disc arthroplasty did not seem to result in more dysphagia complaints. Future studies comparing cervical disc arthroplasty and no-profile fusion devices may help delineate the effect that anterior instrumentation profile has on postoperative dysphagia.
Extended references
Incidence of dysphagia after anterior cervical spine surgery: a prospective study.
Bazaz R, Lee MJ, Yoo JU.
STUDY DESIGN: A prospective longitudinal study was conducted to evaluate dysphagia after anterior cervical spine surgery. OBJECTIVES: To evaluate the incidence and natural history of dysphagia after anterior cervical spine surgery, and to identify risk factors for the development of postoperative dysphagia. SUMMARY OF BACKGROUND DATA: The literature contains only retrospective evaluations of postoperative dysphagia. A wide range of incidence has been reported in these studies. METHODS: Altogether, 249 consecutive patients undergoing anterior cervical spine surgery were eligible for the study. These patients were contacted 1, 2, 6, and 12 months after the procedure to evaluate swallowing. Risk factors such as age, gender, procedure type, hardware use, and number and location of surgical levels addressed were assessed. RESULTS: Dysphagia incidences of 50.2%, 32.2%, 17.8%, and 12.5% were found at 1, 2, 6, and 12 months, respectively. At 6 months after the procedure, only 4.8% of the patients were experiencing moderate or severe dysphagia. Patient age, type of procedure (corpectomy vs. discectomy or primary vs. revision), hardware presence, and location of surgical levels were not statistically significant risk factors for the development of postoperative dysphagia. Female gender was significant for increased risk of dysphagia at 6 months. Surgery at multiple disc levels increased the risk of postoperative dysphagia at 1 and 2 months. The etiology of the dysphagia in most of the patients was unknown. However, vocal cord paresis was identified in 1.3% of the patients at 12 months. CONCLUSIONS: Dysphagia after anterior cervical spine surgery is a common early finding. However, it decreases significantly by 6 months. The minority of patients experience moderate or severe symptoms by 6 months after the procedure. Female gender and multiple surgical levels could be identified as risk factors for the development of postoperative dysphagia.
Dysphagia after anterior cervical decompression and fusion: prevalence and risk factors from a longitudinal cohort study.
Riley LH III, Skolasky RL, Albert TJ, Vaccaro AR, Heller JG.
STUDY DESIGN: Retrospective analysis of the incidence and prevalence of dysphagia after anterior cervical decompression and fusion (ACDF). OBJECTIVES: To examine the incidence and prevalence of dysphagia after ACDF, determine possible associated patient and procedural characteristics, and examine dysphagia's impact on long-term health status and function. SUMMARY OF BACKGROUND DATA: Dysphagia is a common early complaint after ACDF, but the risk factors associated with its development are not understood. METHODS: Telephone surveys (Cervical Spine Outcomes Questionnaire) and clinical assessments (Oswestry Neck Disability Scale and SF-36) were used to evaluate 454 patients who had undergone ACDF at one of 23 nationwide sites for individual and procedure characteristics that might contribute to dysphagia. RESULTS: Of the 454 patients, 30% reported dysphagia at the 3-month assessment (incident cases). The incidence of new complaints of dysphagia at each follow-up point was 29.8%, 6.9%, and 6.6% at 3, 6, and 24 months, respectively. Dysphagia persisted at 6 and 24 months in 21.5% and 21.3% of patients, respectively. The risk of dysphagia increased with number of surgical vertebral levels at 3 months: 1 level, 42 of 212 (19.8%); 2 levels, 50 of 150 (33.3%); 3+ levels, 36 of 92 (39.1%). Patients reporting dysphagia at 3 months had a significantly higher selfreported disability and lower physical health status at subsequent assessments. CONCLUSION: Duration of preexisting pain and the number of vertebral levels involved in the surgical procedure appear to influence the likelihood of dysphagia after ACDF.
Persistent swallowing and voice problems after anterior cervical discectomy and fusion with allograft and plating: a 5- to 11-year follow-up study.
Yue WM, Brodner W, Highland TR.
Anterior cervical discectomy and fusion is commonly performed for cervical disc disease. Most studies report that swallowing and voice problems after such surgeries tend to resolve with time and are often of minor significance except in the rare cases of recurrent laryngeal nerve palsies. A retrospective review was performed on patients who had anterior cervical discectomy and fusion by a single surgeon more than 5 years prior, to determine the persistence of swallowing and voice problems in them. Seventy-four patients who had anterior cervical discectomy and fusion with allograft and plating an average of 7.2 years prior responded to an invitation to return for a follow-up clinical review. Emphasis was placed on the symptoms of dysphagia and dysphonia, as related to the index surgery. At final review, persistent dysphagia was present in 26 patients (35.1%). This occurred more frequently in females and in younger patients. Dysphonia at final review persisted in 14 patients (18.9%). This also occurred more commonly in females and in patients in whom possible non-union is present in at least one of the levels operated upon. Problems with singing were present in 16 patients (21.6%) postoperatively, occurring more frequently if the C3/4 disc was included in the surgery and in patients who have had a greater total number of anterior cervical surgeries at the time of review. Dysphonia and dysphagia are persistent problems in a significant proportion of patients, even beyond 5 years after anterior cervical spine surgery.
Influence of anterior cervical plate design on Dysphagia: a 2-year prospective longitudinal follow-up study.
Lee MJ, Bazaz R, Furey CG, Yoo J.
OBJECTIVE: To compare the incidence, prevalence, and rate of improvement of dysphagia in patients undergoing anterior cervical spine surgery with two different anterior instrumentation designs. METHODS: The study subjects were 156 consecutive patients undergoing anterior cervical spine surgery with plate fixation. We compared the incidence of dysphagia among the two different plate groups both produced by the same manufacturer (Medtronic Danek); the Atlantis plate has thicker and wider plate dimensions than the Zephir plate. Dysphagia evaluations were performed prospectively by telephone interviews at 1, 2, 6, 12, and 24 months following the procedure. Risk factors such as gender, revision surgery, and number of surgical levels were compared between the groups and were not statistically different. RESULTS: Overall incidences of dysphagia were 49%, 37%, 20%, 15.4%, and 11% at 1, 2, 6, 12, and 24 months, respectively. Severe and disabling dysphagia is reported to be a relatively uncommon complication of anterior cervical surgery. However, a significant number of patients report mild to moderate discomfort including double-swallowing and catching sensation. Except at the 2-month follow-up point, the Atlantis plate group had higher incidences of dysphagia than the Zephir group at all time points (57% vs 50%, 36% vs 4%, 23% vs 14%, 17% vs 7%, 14% vs 0% at 1, 2, 6, 12, and 24 months, respectively). The Atlantis plate group had a 14% incidence of dysphagia at 2 years compared with the Zephir group, which had a 0% incidence at 2 years (P < 0.04). For primary surgeries, there was a higher incidence of dysphagia at all time points in the Atlantis group when compared with the Zephir group (58% vs 43%, 35% vs 30%, 22% vs 10%, 17% vs 0%, and 13% vs 0% at 1, 2, 6, 12, and 24 months, respectively) (P < 0.04 at 1 year). A regression analysis was performed. The resulting formulas predict the permanent rate of dysphagia for the Atlantis group is 13.6% and for the Zephir group is 3.58%. CONCLUSIONS: The use of a smaller and smoother profile plate such as the Zephir does reduce the incidence of dysphagia as compared with a slightly larger and less smooth plate such as the Atlantis.
Surgical treatment of dysphagia after anterior cervical interbody fusion.
Fogel GR, McDonnell MF.
BACKGROUND CONTEXT: Dysphagia is a frequent complication after anterior cervical interbody fusion (ACIF). Although dysphagia usually improves over 6 months, it remains a significant and persistent problem for some patients. The etiology is poorly understood but has been reported to be associated with vocal cord paralysis, dislodgement of instrumentation and unidentified causes, such as hematoma, adhesion formation and denervation of the pharyngeal plexus. A surgical treatment of dysphagia after ACIF has not been reported. PURPOSE: We report the surgical treatment of persistent dysphagia occurring after ACIF with instrumentation. STUDY DESIGN/SETTING: A retrospective review of cervical discectomy and interbody fusion patients identified a subset of patients with symptomatic dysphagia who chose surgical treatment of the dysphagia. The hypothesis is that removal of the anterior cervical plate will release mechanical adhesions of the esophagus to the anterior spine around the plate. Outcome was graded by examination and a final telephonic interview with a dysphagia questionnaire. METHODS: Thirty-one patients who elected surgical treatment for persistent dysphagia were assessed at clinic visits after surgery at 3, 6 and 12 months for symptomatic dysphagia, and with a final telephonic questionnaire. The average time from initial surgery to time of surgical treatment for dysphagia was 18 months. Final follow-up was an average 11 months (range, 6 to 25 months) with a dysphagia questionnaire using the Bazaz-Yoo dysphagia score. Thirty-one patients responded to a phone questionnaire with the Bazaz-Yoo dysphagia score. RESULTS: The primary operative finding was extensive adhesions attaching the esophagus to the prevertebral fascia and anterior cervical spine around the periphery of the cervical plate. Seventeen patients (55%) were significantly improved to no dysphagia of solids and liquids (P < or = .0001). Ten patients (32%) reported mild dysphagia occasionally with specific foods. Three patients had persistent moderate occasional dysphagia with solid food. Two patients had persistent severe dysphagia of solids and liquids. Previous cervical surgery, particularly with pre-existing dysphagia, and unexpectedly extreme amounts of adhesions at surgery were contributing factors to the cases with persistent severe dysphagia. CONCLUSIONS: Surgical treatment of dysphagia after ACIF has not been reported. Removal of the cervical instrumentation in patients will improve the dysphagia. This improvement with surgical management, as compared with the dissatisfaction before surgical treatment, documents that this surgical treatment is a reasonable option.
- © 2010 SAS - The International Society for the Advancement of Spine Surgery. Published by Elsevier Inc. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Dr. Jason Datta is a consultant for Synthes.
Dr. Bruce Darden owns stock in Synthes Spine (West Chester, PA) and is a consultant for Synthes and Stryker Spine (Allendale, NJ).
Dr. Daniel Murray is a consultant for Synthes and Stryker, receives royalties from Stryker, and owns stock in US Spine (Boca Raton, FL) and Pioneer Surgical (Marquette, MI).
In this issue




{kind=link}