


Abstract
Background Currently, there are different routines in Norwegian hospitals regarding how recent magnetic resonance imaging (MRI) of the lumbar spine should be performed before surgery. Patients with lumbar spinal stenosis from the Norwegian degenerative spondylolisthesis and spinal stenosis study, who had 2 preoperative MRIs performed within the year before surgery, were included. The aim of the present study was to evaluate the utility of repeated preoperative MRI for patients undergoing decompressive spine surgery for degenerative spinal stenosis.
Methods For all included patients, the changes between the 2 preoperative MRIs were investigated for disc degeneration (Pfirrmann’s classification), foraminal stenosis (Lee’s classification), spondylolisthesis, and central canal stenosis (Schizas score and dural sac cross-sectional area).
Results A total of 65 patients (78 levels) were included. Thirty-seven patients were women, and the mean age was 67 (range 48–79) years. Schizas score showed a clinically meaningful change of ±2 or 3 grades in 5 levels, and dural sac cross- sectional area was reduced in 47 levels with a mean change of −2.3 mm2. Three levels had a clinically relevant change in grade of foraminal stenosis of ±2. For disc degeneration, 53 of the levels had no change, and the rest of the levels had a change of ±1 grade. Increased spondylolisthesis was measured at 21 levels, and the mean slip was <2 mm. Also, 4 levels had >2 mm slip.
Conclusion For patients undergoing surgery for lumbar spinal stenosis, repeated MRI within the year before planned surgery showed few significant changes in common radiological parameters. The benefit for the surgeon of repeat MRI is therefore limited.
Level of Evidence 2.
INTRODUCTION
Degenerative lumbar spinal stenosis (LSS) is described as a condition with diminished space available for the neural and vascular elements in the lumbar spine, secondary to degenerative changes in the spinal canal.1 LSS mainly affects the elderly population, and due to an aging population, the prevalence of LSS is increasing. Symptomatic LSS is currently one of the most frequent causes for lumbar spinal surgery.2,3 The diagnosis of LSS is made by clinical symptoms with corresponding radiological findings. Typical symptoms for LSS are increased frequency of low back pain and discomfort, as well as radiating pain to 1 or both lower limbs when standing or walking.4
Magnetic resonance imaging (MRI) is the recommended imaging modality for diagnosing LSS. A consensus regarding distinct radiological criteria to quantify and describe spinal stenosis has not been reached, neither how to assess diagnostic performance nor how to compare images from different imaging modalities.
In Norway, MRI imaging is routinely done before LSS surgery, but there is a lack of consensus between hospitals of how current these images should be at the date of surgery. From our experience, if the images are older than 6 to 12 months at the date of surgery, new images are taken before surgery.
The aim of this study was to evaluate the usefulness of repeated MRI, within the preceding year before LSS surgery, for patients with or without degenerative spondylolisthesis. We hypothesized that routine repeated MRIs would not show clinically significant changes in common selected radiological parameters and would not lead to any change in the preoperative plan.
METHODS
Study Population
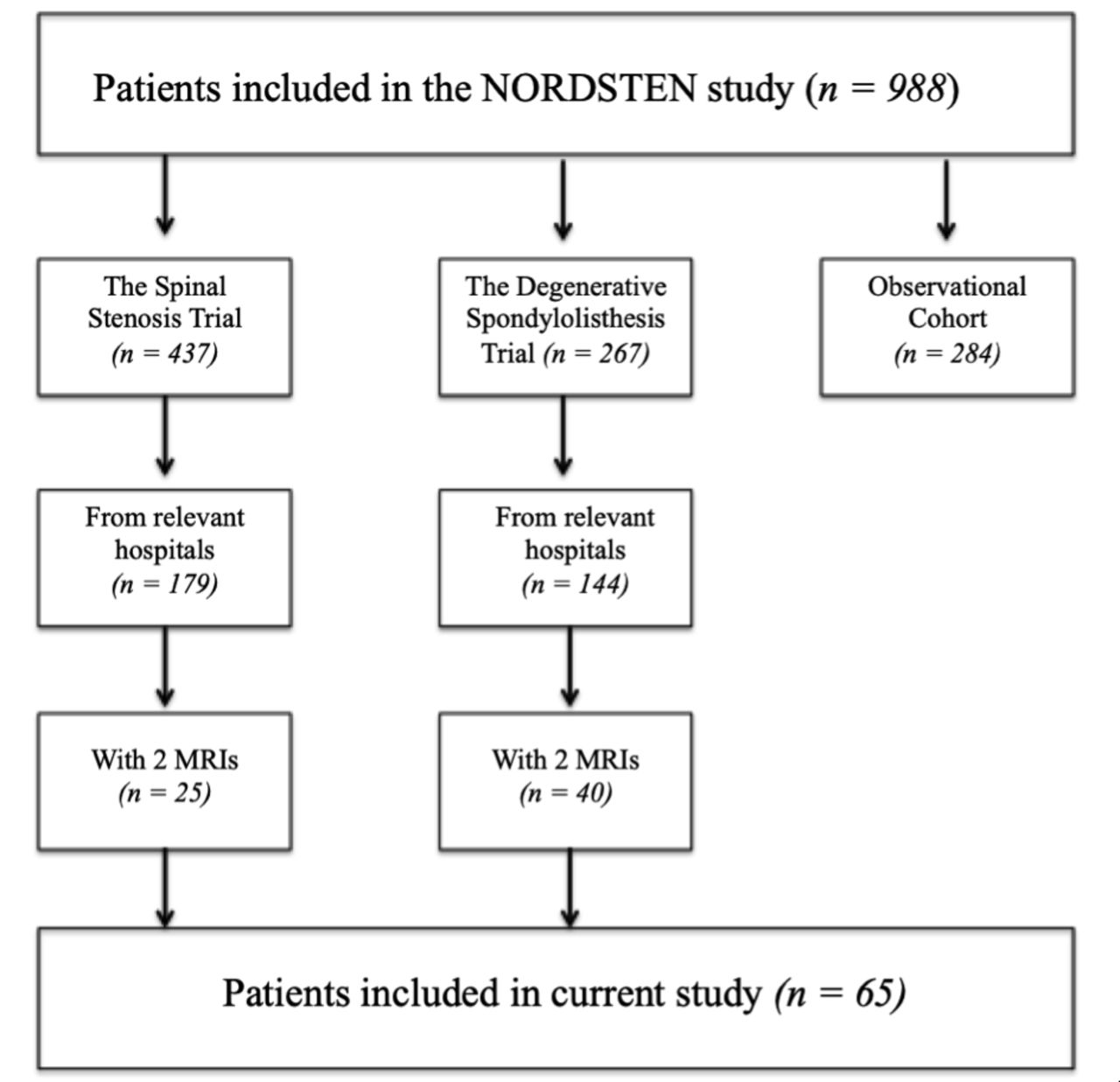
Patient data were retrieved from the Norwegian degenerative spinal stenosis study (the NORDSTEN study) where 988 patients from 16 Norwegian hospitals were prospectively included from 2014 to 2018. The NORDSTEN study has 3 arms: the spinal stenosis trial, the degenerative spondylolisthesis trial, and an observational cohort.5–7
In the current study, patients were included from the 3 major contributing hospitals in the spinal stenosis trial and degenerative spondylolisthesis trial.5–7 The patients should have 2 preoperative MRIs performed within the previous year before the planned date of surgery. According to the study protocol for the NORDSTEN study, it was mandatory for the patients to have a recent MRI (at least 6 months prior to inclusion). One of the 2 MRIs was therefore performed less than 6 months before the planned date of surgery. The MRI records for all patients were retrospectively reviewed to identify all eligible patients. This gave a total study population of 65 patients (Figure).
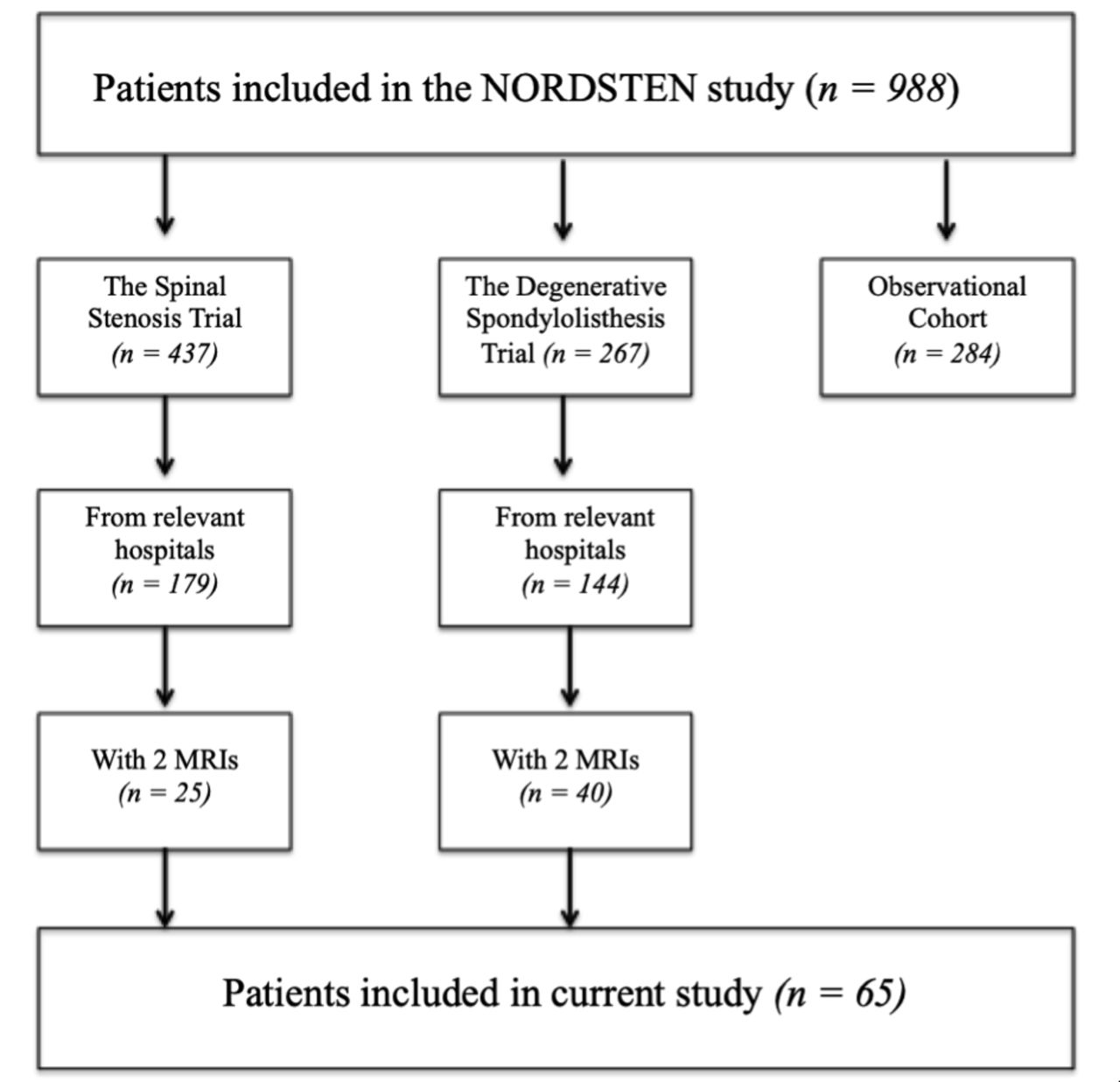
Patient selection. MRI, magnetic resonance images; NORDSTEN study, the Norwegian degenerative spinal stenosis study.
Radiological Measurements
All patients in our study had axial T2-weighted images in addition to sagittal T1- and T2-weighted images of the lumbar spine. In the current study, we chose to evaluate 7 of the most common parameters to compare the severity and development of the degenerative stenosis between the 2 MRIs performed in the individual patients: central canal stenosis with Schizas qualitative grading (grade A–D) based on the morphology of the dural sac,8 and as dural sac cross-sectional area (DSCA) measured in square millimeter at the narrowest point in the spinal canal. If DSCA area is <75 or <100 mm2, the stenosis is considered severe or moderate, respectively.9–11 Foraminal stenosis was evaluated by Lee et al’s classification from grade 0 to 3.12 To evaluate the intervertebral disc degeneration, the classification from Pfirrmann grade 1 to 5 was used.13 Spondylolisthesis was measured on the pathologic level(s). Any slip was rounded off to the nearest full millimeter measured. The measurements were performed at level L2-L5. All measurements were performed twice by an experienced musculoskeletal radiologist and an orthopedic surgeon with >10 years’ experience in spinal surgery. A mean was calculated for all continuous parameters, while a majority count was calculated for categorical parameters in cases of disagreement. Reliability studies have been conducted between orthopedics and radiologists in the NORDSTEN study, and the relevant parameters have shown good or very good agreement.14
Statistical Methods
Mean and corresponding SDs were used to describe continuous MRI measurements. Paired sample t tests were used to test for differences in means between the 2 measurements. For categorical outcomes, frequencies and relative frequencies were presented. All tests were 2-sided, and the significance level was set to standard 5%. All analyses were done using SPSS version 25.0 (IBM Corporation, Chicago, IL, USA).
RESULTS
There were 65 patients and 78 levels examined: 52 patients were scheduled to undergo surgery at 1 level, 12 patients at 2 levels, and 1 patient at 3 levels. The investigated levels were: 2 in L2-L3, 22 in L3-L4, and 54 in L4-L5. The patients had a mean age of 67 years (range 48–79 years), and there were 37 women.
Radiological Results
The time between the first and second MRI was in average 231 days. The changes in radiological measurements are presented in the Table. For all parameters, there were no clinical meaningful changes.
Changes between the first and second MRI measurements of 65 patients who were scheduled for decompressive surgery in a total of 78 levels due to lumbar spinal stenosis.
Schizas showed no change in 50 of 78 levels. The mean change at all pathological levels was 0.32. The average change at the levels where a change occurred was 0.69.
DSCA showed no change or improvement in measurements in 50 of 78 levels. Mean measured DSCA from initial to repeated MRI showed minimal change with a reduction of −2.3 mm2, from 56.54 to 54.24 mm2. When assessing the progression of the stenosis, 55 levels were already classified as severe stenosis at the initial evaluation and remained within this category on the repeat MRI. From the initial MRI examination to the repeat MRI, 2 levels were classified as nonstenosis but developed to moderate stenosis, and 6 levels classified as moderate stenosis on the initial MRI developed to severe stenosis.
Foraminal stenosis, on both right and left sides, showed no change or improvement in measurements in 140 of 156 levels. Three levels had a clinically meaningful stenosis change of ±2. Disc degeneration showed no change or improvement in measurements in 66 of 78 levels. Spondylolisthesis showed no change or improvement in measurements in 57 of 78 levels. The average slip was <2 mm. Four levels had increased sliding >2 mm.
DISCUSSION
In the present study, we observed few changes in the radiological evaluation of degenerative LSS when selected common radiological parameters were measured on 2 MRI examinations taken the preceding year before decompressive spinal surgery.
Our findings were consistent with Lee et al15 who explored the benefits of repeat preoperative MRIs for patients with LSS and concluded, based on central canal stenosis (Schizas) and foraminal stenosis (Lee’s classification), that repeated MRIs within 1 year had low value. The same study defined that a clinically meaningful change for central canal or foraminal stenosis was a change of 2 or 3 steps in the score. When using the same limits in the current study, there were few levels that had changes of clinical relevance. There is limited published literature on the current topic, but in a study by Keshtkaran et al,16 it is also described that repeat preoperative lumbar MRIs were considered unnecessary if an MRI is performed within the past year unless new neurological symptoms had occurred.
In the present study, the changes of several other radiological parameters commonly used in the diagnosis of spinal stenosis as DSCA, disc degeneration, and spondylolisthesis were measured. These parameters also had minimal changes from the initial to repeated preoperative MRI; thus, it seems that a repeated MRI immediately before surgery for LSS has little clinical benefit.
There is a controversy about to what extent the compression of the dural sac measured as DSCA is related to the clinical symptoms of LSS.6–8 Nevertheless, DSCA is considered to be one of the most common measurements in the radiological diagnosis of LSS.10 Many levels showed reduction of DSCA during the period between MRI examinations. However, the average reduction of 2.3 mm2 is considered minimal, and this is not considered to have clinical relevance. The majority of the levels were already classified as severe stenosis in initial MRI, none of the levels went from no to severe stenosis, and just 6 of the levels went from moderate to severe stenosis.
An association between the clinical symptoms and the radiological findings of LSS is not always present.17 Nevertheless, both the clinical symptoms and the radiological findings are considered important in the preoperative assessment of the patient with LSS. In the present study, all patients were candidates for spinal surgery. There were minor radiological changes found between the 2 preoperative MRIs, and since the changes were not considered clinically relevant, this will probably not result in any alterations in the planned surgical procedure.
The finding of both increased and decreased measurements of stenosis degree can likely be explained by measurement uncertainty. To ensure the least possible measurement uncertainty in the radiological measurements in the NORDSTEN study, all orthopedic surgeons and radiologists who performed radiological measurements were agreed on measurement methods.
One limitation of our study was that we did not know whether the new preoperative MRI images were based on changes in symptoms or as a routine to get a “fresh” MRI before surgery. In Norway, there are no legal issues that prompt us to order new images within 6 months before surgery, but this can be the issue in other countries. Nevertheless, worsening of symptoms should always lead to consideration of a new MRI. If the reason for a second MRI was worsening of symptoms, for instance, with increase of degenerative spondylolisthesis, this would strengthen our conclusion. Another limitation of our study is the relatively small number of patients.
CONCLUSION
For patients scheduled for decompressive surgery due to LSS, repeated MRIs of the lumbar spine showed few surgically relevant radiological changes in central spinal canal stenosis, foraminal stenosis, disc degeneration, and spondylolisthesis. The results of this study suggest that in the absence of aggravated symptoms, new routine MRI images taken just before surgery are not required if images were taken in the past year.
Footnotes
Funding Sophies Minde Foundation in Norway, grant number 02/2019.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethical Approval The Norwegian Committees for Medical and Health Research Ethics (2011/2034 and 2013/366) approved the study. The patients have signed a written, informed consent as part of their inclusion in the NORDSTEN study.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}