


Abstract
Background Pressure measurements to detect risks for pressure injuries in wheelchair users with spinal cord injury (SCI) have been available for quite some time. Unfortunately, knowledge of how postural changes during longer periods of daily life activity affecting the results is still limited. In the present study, the authors expected to note shifts in the center of pressure as well as in the pressure distribution, especially in patients who were able to change their position actively.
Methods A seat pressure mat (BodiTrak2) was used to perform measurements of 34 SCI wheelchair users after initial transfer into the wheelchair as well as 30 and 90 minutes later. Mean pressure, maximum pressure, pressure-loaded measuring surface, and the coordinates of the center of pressure were analyzed, and findings were statistically analyzed using the t test and Intraclass Correlation Coefficient. To quantify the drift of the measurement system, recordings with a reference weight were performed.
Results The analyzed parameters from the initial measurement differed significantly from the later measurements at 30 and 90 minutes, whereas the parameters were stable after 30 minutes. The measurements with the reference weight showed the same measurement course.
Conclusions The measurements after 30 and 90 minutes were consistent, contrary to expectations. The activity of the participant between measurements did not appear to be of much importance.
Clinical Relevance Relief maneuvers appear to provide relief only while the maneuver is being performed. Thus, relief activities must be frequent enough and long enough to allow adequate blood flow to the tissues.
Introduction
Pressure injuries are a serious secondary complication of spinal cord injury (SCI).1–4 It is one of the challenging tasks of clinicians to observe repeated development of pressure ulcers in patients despite all kinds of efforts—on both the patients and therapist’s side. The development of pressure ulcers is influenced by a variety of factors, including extrinsic factors such as pressure, shear/friction, positioning, and load duration, but also intrinsic factors such as age, weight, blood pressure, continence, and immobility. Among all these factors, pressure and load duration have been discussed to be the primary contributors to the development of pressure ulcers.5–9 It is true that the skin can tolerate high pressures for a short time. However, if this pressure is maintained for a longer period, capillaries can be compressed and hypoxia and even necrosis may occur due to reduced tissue perfusion.7 The average tolerance range of the skin to pressure stress and the time of pressure exposure varies individually from 30 to 240 mm Hg.7 Pressure above the limit at which the individual can tolerate over a prolonged period is very likely to cause pressure ulcers.10 These mechanisms are well recognized, and a lot of research has been placed into the detection and possible prevention of these adverse conditions.
One of the research targets has been the development of pressure measurements while participants sit still. Pressure distribution within the seating surface can be measured using a seating pressure mat.11–14 Studies about the stability of sitting pressure measurements were often carried out on healthy participants.11–13 In these studies, measurements were performed regularly over a period of 20 minutes. It was remarkable that measured values were only stable after a certain period. Therefore, it was recommended that the first measurement be taken between 212 and 613 minutes after positioning the participants. In another study, which included both wheelchair-dependent and non-wheelchair-dependent participants, a waiting time of 8 minutes was suggested.15 However, it has never been addressed how activities of everyday life (eg, moving in the wheelchair or pushing the wheelchair) alter the pressure distribution. For example, nobody could tell what a measurement, taken after some time of regular activities, would look like considering the peak pressures and their distribution depending on positioning and posture in the wheelchair. It is not even known if and how much change in these parameters are desirable or which ones might be detrimental. Clinical prevention strategies include both regular shifts and unloading to improve capillary blood flow as well as individualized cushions to protect vulnerable “localized” pressure zones.
Currently, it is largely unknown how stable sitting pressure measurements are over a prolonged period and how well the measurement protocols reflect the actual load in everyday life. Thus, we decided to repeatedly perform seat pressure measurements with wheelchair users after some time of regular activities. We hypothesized that a measurement after 30 and 90 minutes of everyday activities would reveal notable changes in pressure (ie, maximum pressure, mean pressure, pressure-loaded measuring surface, as well as the coordinates of the center of pressure), especially in patients who were able to change their position actively.
Methods
Participants
Participants with SCI were recruited as part of the routine examination by a qualified occupational therapist who performs seating pressure measurements on patients at the SCI Unit at Klinikum Bayreuth GmbH (Hohe Warte), Germany. Patients who were older than 18 years and wheelchair-dependent were included. Exclusion criteria were severe cognitive impairments that precluded participation. Informed written consent was obtained from each volunteer participant. The investigation was approved by the ethics review board of the Friedrich-Alexander University Erlangen-Nuremberg, Germany (application number 480_18B) and was in accordance with the Declaration of Helsinki.
An a priori power analysis for an analysis of variance model conducted by means of G*Power 3.1.5 software revealed the necessity of 34 participants given the following input parameters: effect size F = 0.4 (detectable), alpha error probability: 0.05, power: 0.8, and number of groups: 1. To gather the relevant information about the characteristics of the participants, we collected their weight, height, age, gender, level and severity of lesion (American Spinal Injury Association Impairment Scale), behavior in the wheelchair (ie, able or unable to reposition themselves in the wheelchair as needed and desired), and cushion type.
Data Acquisition
Measurements were taken using a pressure mat (BodiTrak2, 16 × 16 = 256 piezoelectric sensors)16,17 placed on the seat cushion in the wheelchair (Figure 1). To represent the conditions of everyday life, the participants used their own wheelchair as well as their own cushion. Using the standard supplied FSA.1 software package (BodiTrak, Winnipeg, Canada), the following relevant parameters were measured for all participants and the reference weight: maximum pressure (mm Hg), mean pressure (mm Hg), measurement area (cm2), as well as the coordinates of the center of pressure (cm).

Measurement setup. Measurements were taken using a pressure mat (BodiTrak2, 16 × 16 = 256 sensors) placed on the participants own seat cushion in their own wheelchair. Using the standard supplied FSA.1 software package, the following parameters were measured: maximum pressure (mm Hg), mean pressure (mm Hg), measurement area (cm2) as well as the coordinates of the center of pressure (cm).
Reference Measurement
Measurements were performed with a reference weight (10 kg kettlebell) to standardize the measurements and to better evaluate the stability of the measurements. The weight measurements also eliminated some confounding factors such as movement between measurements or folding of clothing. The weight was placed in the middle of the mat for 90 minutes. During this time, measurements were taken every 5 minutes. The described procedure was performed with 3 different cushions to identify whether any differences existed between the cushion types: KUBIVENT DualPlus, KUBIVENT TheraCubus, and ROHO Dry Floatation wheelchair cushion. These 3 cushions were the most common among the participants.
The measurements with the KUBIVENT DualPlus cushion were performed 5 times. The results (regarding reliability) of the examination of this measurement course under identical conditions allowed it to measure with the other 2 different cushions (KUBIVENT TheraCubus and ROHO Dry Floatation) once each. The evaluation of the pressure mean values was first performed of the 5 measurement repetitions with the KUBIVENT DualPlus cushion using a 2-tailed t test for 2 dependent samples with P = 0.05. The pressure mean values were normally distributed according to the Shapiro-Wilk test (P = 0.05). In addition, reliability of the maximum pressure, the pressure mean values, the pressure-loaded measurement surface, and the coordinates of the center of pressure were assessed using the calculation of Intraclass Correlation Coefficients (ICCs) with an ICC(2,1) model.18 ICC values were interpreted as follows: >0.75 was excellent, 0.60 to 0.74 was good, 0.40 to 0.59 was fair, and <0.40 was poor.19 The results allowed it to perform the same statistical calculations also for the evaluation of all the 3 cushions together that are the 5 measurement repetitions with the KUBIVENT DualPlus and the individual measurements each with the KUBIVENT TheraCubus and the ROHO Dry Floatation wheelchair cushion.
To complement the evaluation of the 5 measurements with the KUBIVENT DualPlus cushion, the mean value and the SD of all pressure mean values from minute 0 to 90 of the 5 measurements were also calculated. Furthermore, the SD of the pressure mean values over all 5 measurements with the KUBIVENT DualPlus cushion were calculated for minutes 0, 30, and 90.
Measurements of the Wheelchair-Dependent Participants
Prior to the first measurement, all participants were positioned with the iliac crest horizontal, the hip joints in flexed but neutral position without external or internal rotation and forward pointing kneecaps. Subsequently, they remained in their wheelchair for the duration of the study and were encouraged to move as desired and in accordance with the necessities of their activities. They were also asked to perform pressure relief maneuvers as usual (eg, leaning to the side or pressing up).20 For the further measurements, the participants maintained their current sitting position and were not repositioned by the therapist.
Three measurements were taken: measurement 1 usually 2 to 4 minutes after positioning on the mat (minute 0), measurement 2 at 30 minutes, and measurement 3 at 90 minutes. The Clinical Guidelines for the Use of Interface Pressure Mapping for Seating were applied when performing the seated pressure measurements. The analysis of the participant’s measurements was conducted first for all participants together and second for the 2 subgroups: participants who can change their position actively and participants who were not able to change their position actively. The evaluation was conducted for all groups in the same way.
To evaluate the participant measurements (ie, maximum pressure, pressure mean value, pressure-loaded surface, and vertical and horizontal coordinates of the center of pressure), we performed a 2-tailed t test for 2 dependent samples (minute 0 vs minute 30, minute 0 vs minute 90, and minute 30 vs minute 90) with P = 0.05. Means were normally distributed according to the Shapiro-Wilk test (P = 0.05). In addition, reliability was assessed using the calculation of ICCs with an ICC(2,1) model.18 All data were analyzed using IBM SPSS Statistics version 26.
Results
A total of 34 participants were included in the present study. Most participants were men and were active in their wheelchairs. The mean age was 47.5 years (Table 1). For participant-specific information, view Supplementary Material 1.
Participant characteristics.
Supplementary Material 1.
Reference Measurements
Both the t test and the ICC show that the reliability of the 5 measurements with the KUBIVENT DualPlus cushion is given. The pressure mean values at minutes 0 and 30 were not consistent; they deviated strongly from each other. The pressure mean values at minutes 30 and 90 were consistent. Furthermore, the pressure-loaded measurement surface changed only slightly between the measurements. These results proving the identical stable measurement conditions allowed the evaluation of all 3 cushions together (KUBIVENT DualPlus, KUBIVENT TheraCubus and ROHO Dry Floatation). Also, in the following common evaluation of the measurements of all 3 cushions, the reliability is given, and the results stayed stable as well (Table 2).
ICCs of the seat pressure measurements.
Mean ± SD of the seat pressure measurements.
We evaluated the 5 measurements with the KUBIVENT DualPlus cushion with respect to the mean values and SDs of all pressure mean values from minutes 0 to 90. The mean (SD) values of all pressure mean values from minutes 0 to 90 showed an outlier in the fourth measurement but were otherwise constant. The absolute measured mean (SD) pressure values of the measurements at minutes 0, 30, and 90 changed with each new measurement but were constant over the course of a measurement from minute 0 to 90. The SD of the pressure mean values was 14.16 at minute 0, 13.75 at minute 30, and 9.79 at minute 90. Furthermore, the SD became smaller in the course of minute 0 to minute 90. In summary, these results also support the results obtained above.
Measurements of the Wheelchair-Dependent Participants
The statistical evaluation of the results of the participant measurements confirmed the results of the simulation with a 10 kg reference weight (Tables 2 and 3). The pressure mean value and the pressure-loaded measuring surface at minute 0 differed from the measurements at minutes 30 and 90. Both the t test and the ICC proved that the pressure mean value and the pressure-loaded measuring surface after 30 minutes (between minutes 30 and 90) were stable and did not differ significantly (Tables 2 and 3; Figure 2). These results can be obtained also in the active subgroup and partly in the inactive subgroup. Additionally, the maximum pressure and the horizontal and vertical coordinates of the center of pressure did not differ significantly between the 3 measurements and showed excellent reliability after 30 minutes (Tables 2 and 3).

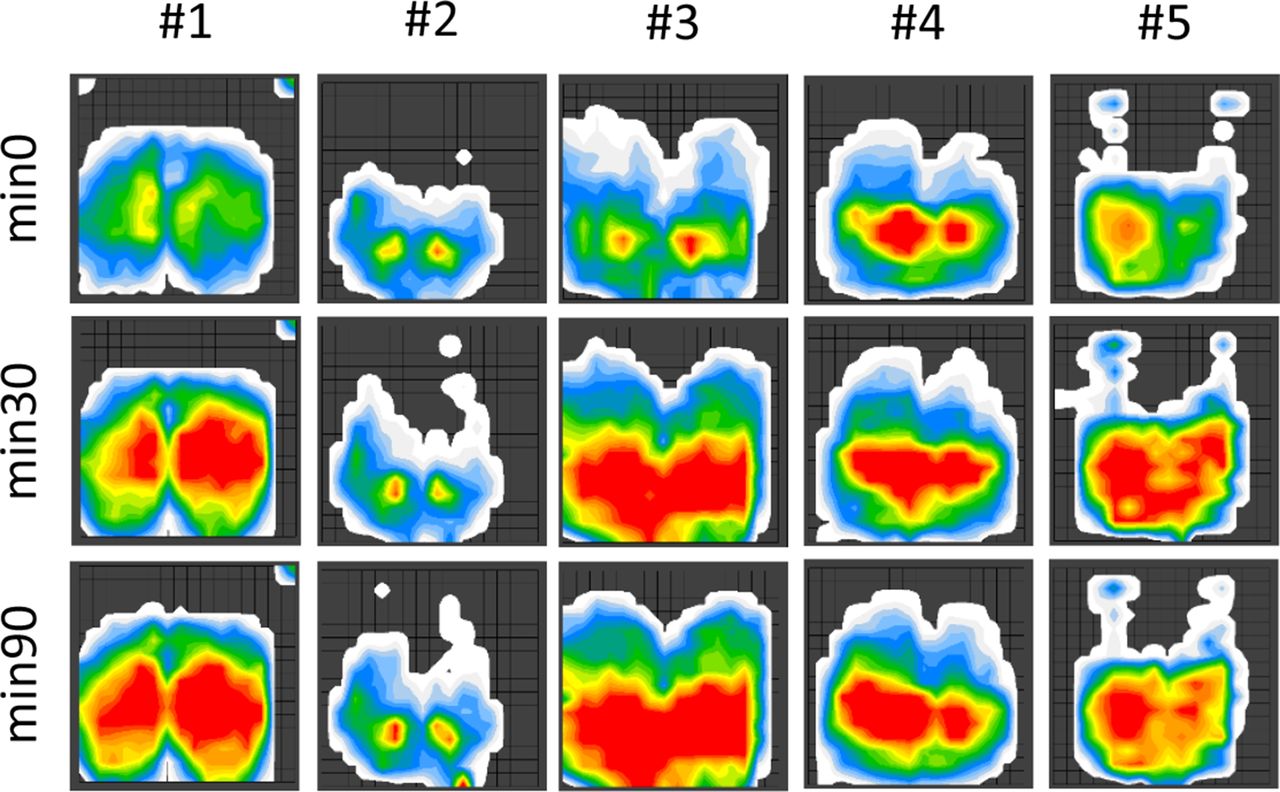
Examples of a seat measurement. Examples of a seat measurement at minute 0, at minute 30, and at minute 90 for 5 active spinal cord injury participants.
Discussion
Since pressure measurements are a way to assess the risk of pressure injuries, we first wanted to make sure that the measurements were reliable. This is especially important because treatment decisions concerning the use of cushions are often based on the pattern retrieved from pressure measurements.
In clinical practice, seating pressure measurements are performed by placing the measurement mat between the participant and the cushion of the wheelchair. Usually, this measurement is performed once the participant sits “well,” at least in the eyes of the person performing the test. Dangerous pressure loads are assumed if zones are found in which pressure limits are exceeded. They are usually shown with a red color coding (see Figure 2). However, there were no good data available regarding whether this measurement was valid and representative while the participant carries out his or her usual activities and moves in the wheelchair in the usual load situation and according to the individual’s paralysis situation and body position. Thus, we hypothesized that a measurement after 90 minutes of everyday activities would reveal notable changes in peak pressure areas and the center of pressure. In contrast to our expectation, the values of the participant measurements at minutes 30 and 90 were very similar and comparable to the reference measurements using a static weight (Tables 2 and 3). This result does not support the notion that different areas of tissue are under pressure after most repositioning maneuvers.
Moreover, both active and inactive participants had nearly the same results (Tables 2 and 3). These results have considerable clinical significance. In many SCI units, pointing out the importance of regular offloading to prevent pressure damage is a core part of guiding patients. Patients with recurrent pressure injuries are not infrequently even blamed for causing the problem themselves. However, this view is difficult to reconcile with our results. The aim of unloading is to bring the patient into a different sitting position in order to restore the blood supply to the tissue areas in the zones of highest pressure. Apparently, however, this does not happen. Therefore, patients should at least be advised to perform the unloading maneuver long enough to ensure blood flow.
Sitting pressure measurements were also performed in such a way that participants were repositioned each time between measurements. For example, Meiners repositioned 10 paraplegic participants on 4 different seat cushions each time between measurements and measured highly reliable values with a total of 10 measurement repetitions.21 In another study that took place over 74 minutes, the pressure distribution on different seat cushions for 8 healthy participants was investigated. However, pressure mean values and peak values showed only very small, nonsignificant changes over the measurement period for all variants.14 Both the study by Meiners21 and our study indicate that participants repeatedly come to the same sitting position, regardless of whether they actively move between measurements while remaining seated on the wheelchair, as in this study, or whether they are repositioned between each measurement.21
This is a very important finding for the clinician as relief maneuvers appear to provide relief—and improved blood flow—only while the maneuver is being performed. The additional benefit of a change in position, which distributes the pressure to different areas of the skin, is negligible. Thus, relief activities must be frequent enough and long enough to allow adequate blood flow to the tissues, and activities that result in weight shifts (eg, leaning forward or sideways) should be encouraged.
To prevent patients from returning to the same position following relief maneuvers, recent studies have investigated the use of systems for continuous measurement of interface pressure in SCI patients.22–26 These measurement systems have the potential to inform the development of feedback systems22,24,26 that could improve the regularity of an individual’s relief activities and ultimately reduce the risk of developing pressure ulcers. With such a system, measurements would then also be possible over a longer period of time (days and/or weeks) than in our study. Additionally, if patients are unable to perform sufficient relief activities, the feedback could be used to automatically adjust the pressure distribution in the seat cushion.27,28
Limitations
Measurements are prone to being disturbed by positioning, movements of the test persons, folds of clothing, different elasticity of seat cushions, and the measuring mat and the stretching of the mat. For example, it can only be assumed how the stiffness of the mat itself distorts the measurements. Furthermore, the slowly changing pressure due to the inertia of the pressure sensors affects the measurement results. The error due to the inertia of the pressure sensors decreases over time, and reliable results are obtained. The pressure measurement sensors settle with respect to the measured pressure. Thus, with longer waiting, the error can be sufficiently reduced due to the inertia of the pressure measurement sensors. Nevertheless, it is difficult to say, especially at the beginning of a 90-minute measurement, whether the participants did not move during the measurement or whether the pressure sensors were too inert. Additionally, no maximum pressure values beyond 200 mm Hg could be measured (ie, the sitting pressure mat [BodiTrak2] is not able to measure pressure over 200 mm Hg and the system cannot be scaled to the participants weight). This means that pressure values beyond 200 mm Hg are ignored when calculating the coordinates of the center of pressure. However, the effect on the center of pressure calculation is unknown and should be taken into account in future studies.
Conclusion
Treatment options to minimize the risk of pressure injuries are often very expensive, and resources are limited. Therefore, it is important to be able to accurately identify patients who need preventive measures.29 The role of static pressure as measured by the mat systems should not be overestimated,10 and individual risk factors must always be taken into account.29 Thus, additional research is necessary to define and manage relevant risk factors.
Acknowledgments
We would like to thank all of our participants for the time they spent doing the pressure measurements. The present work is part of the doctoral thesis of Clara Oette in the frame of obtaining the Dr Med degree at the Heidelberg University Hospital.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Statement of Ethics The ethics committee of the Friedrich-Alexander University Erlangen Nuremberg raises no objections to the conduct of the study (application number 480_18B).
Data Availability Statement The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.