


Abstract
Background The International Society for the Advancement of Spine Surgery hosted the first of a series of 4 webinars on endoscopic spine surgery techniques, focusing on end§oscopic discectomy, foraminotomy, instrumented endoscopic fusion, standalone lumbar interbody fusion with innovative materials, and the role of patient feedback in awake procedures. This series aims to share knowledge and discuss the complexities and clinical evidence of modern endoscopic spine surgery.
Objective To analyze the level of surgeon endorsement for the presented endoscopic spine surgery techniques before and after the webinar, utilizing polytomous Rasch analysis, and to evaluate the potential for these insights to inform clinical guideline recommendations.
Methods A survey was available to 1311 potential respondents during the Zoom webinar, collecting data on surgeon endorsements using a Likert scale. The polytomous Rasch model was employed to analyze responses, considering the complexity of decisions against surgeon expertise, developing a logarithmic measurement scale, allowing objective statistical analysis of categorical variables, highlighting incongruent or out-of-order items vs congruent and in-order items, and driving improvement in clinical guidelines.
Results All 4 topics received higher confidence ratings demonstrated by descriptive statistics, highlighting the webinar’s effective role in surgeon education and in identifying ongoing trends in spine surgery. The logarithmic transformation of these data during Rasch analysis showed noticeable shifts in surgeon confidence levels postwebinar, with increased endorsement for transforaminal full-endoscopic thoracolumbar interbody fusion for hard disc herniation and standalone endoscopic lumbar interbody fusion. The Wright plot and person-item map analyses demonstrated that the webinar effectively targeted areas of initial low confidence, significantly impacting surgeons’ perceptions. Disordered endorsement thresholds remained in the topics of uniportal transforaminal discectomy/foraminotomy and patient feedback during endoscopic spine surgery, indicating issues in response category discrimination or confounding factors not captured by the survey. Ongoing controversies were highlighted by the influence of confounding factors, stemming from preconceived notions and limited familiarity with high-grade evidence.
Conclusion The first in the 4-part webinar series effectively shifted professional confidence and acceptance of innovative surgical approaches among spine surgeons. Observations indicated a high level of interest in applying the endoscopic surgery platform with other advanced technologies. The polytomous Rasch analysis provided nuanced insights into ongoing trends and areas in need of further clarification.
Clinical Relevance Assessing surgeon confidence and acceptance of endoscopic spinal surgeries using polytomous Rasch analysis.
Level of Evidence Level 2 (inferential) and 3 (observational) evidence because Rasch analysis provides statistical validation of instruments rather than direct clinical outcomes.
- Endoscopic spine surgery
- ISASS
- polytomous Rasch analysis
- surgeon endorsement
- patient feedback
- clinical guidelines
- transforaminal discectomy
- foraminotomy
- interbody fusion
INTRODUCTION
The International Society for the Advancement of Spine Surgery (ISASS) recently hosted the first of a series of 4 webinars focusing on the cutting edge of endoscopic spine surgery. The webinar subject for the present article, which is part of an ongoing effort to disseminate knowledge and foster discussions around innovative endoscopic spinal surgery techniques, was centered on the pivotal themes of endoscopic discectomy, foraminotomy, instrumented endoscopic fusion across the thoracolumbar junction for calcified disc herniations, standalone lumbar soft interbody fusion with allograft corticocancellous bone enriched with platelet-rich plasma and mesenchymal stem cells, and the crucial role of patient feedback during awake endoscopic spine procedures. The insights gained from the presentations and the associated discussions were recorded using a survey with 4 questions regarding each lecture. Polytomous Rasch analysis was used to understand better the level of endorsement for each of the presented topics and procedures not only to underscore the rapid advancements in minimally invasive spine surgery but also to highlight the nuanced complexities and strength of the available clinical evidence of the various patient-centric approaches that define modern endoscopic spine surgery practices. This research approach allows for a detailed examination of the perceptions, experiences, and outcomes reported by participants in the ISASS webinar series. It provides a robust framework to evaluate the effectiveness and patient satisfaction associated with endoscopic spine surgery techniques, which could ultimately inform clinical guideline recommendations.
The Rasch model,1–8 rooted in item response theory, provides an advanced framework based on the probabilistic dimensions of choices by considering the interplay between task difficulty and proficiency. In the present study, the authors employed it as an examination tool of partial agreement analysis to objectively analyze the level of endorsement for the 4 topics that were presented during this first of 4 webinars.8 Spine surgery is a largely experience-based surgical subspecialty, where decisions are influenced by a wide array of factors, including patient conditions, surgeon skill, and external variables. Thus, conventional descriptive statistical analysis methods of patient self-reported outcome measures or surgeon decision-making typically do not capture the desired information well. The need for a more sophisticated analytical tool is evident, and the Rasch model fills this gap. It treats categorical data, like Likert-scale survey responses, with a mathematical approach that yields several advantages in evaluating surgeons’ opinions and decisions:
Evaluating complexity and expertise: Unlike traditional methods that assess decisions as merely correct or incorrect, the Rasch model evaluates the complexity of each decision against the surgeon’s expertise. This produces a granular understanding that reflects real-world scenarios more accurately.
Developing a precise measurement scale: Ordinal data from surveys gain an interval-level scale through the Rasch model, enhancing the accuracy of comparisons among surgeons or teams and facilitating professional growth and benchmarking.
Ensuring measurement consistency: A key feature of the Rasch model is its ability to create a consistent scale for measurement, enabling reliable comparisons across varied surgical decisions and patient cases by ensuring that the scale’s validity is not dependent on the specific items assessed.
Highlighting incongruent items: The model identifies items that do not align with expected patterns, pinpointing areas where a surgeon’s decision-making deviates from established norms. This helps refine evaluation tools for better assessment of surgical judgment and expertise.
Driving improvement and guideline enhancement: Insights from Rasch analysis are invaluable for educational initiatives, professional development, and the evolution of clinical guidelines. By uncovering specific decision-making strengths and weaknesses, targeted educational programs and clinical guidelines can be developed to improve surgical outcomes.
By leveraging the polytomous Rasch model,8 the present article aims to distill the expert opinions presented during this webinar’s presentations into actionable insights that can be used to assess the strength of the clinical evidence via surgeons’ responses. Furthermore, the authors aimed to summarize the findings into clinical guidelines by exploring how these advanced surgical techniques are perceived by spine surgeons and assess their potential implications for patient care. This study also ranks the importance of patient feedback during surgery, examining how real-time communication between patient and surgeon can influence intraoperative decision-making to affect surgical outcomes and enhance patient satisfaction. In essence, this article comprehensively explores the clinical value of the latest advancements in endoscopic spine surgery, as shared by leading experts in the ISASS webinar series. Through the lens of polytomous Rasch analysis, the authors seek to psychometrically uncover the depth of surgeons’ knowledge and experience in patient-centric care models that these techniques embody, offering valuable insights into their future adoption, implementation, and impact on spine surgery practice.
MATERIALS AND METHODS
Surgeon Survey
The authors distributed an online survey via www.typeform.com to 1311 potential surgeon respondents via a link available during the ISASS-sponsored Zoom webinar on 27 February 2024. Surgeons were asked to indicate their level of endorsement or the degree of importance of the 4 topics presented during the webinar using a Likert scale from 1 (low) to 5 (high). The survey was administered at both the beginning and end of the webinar to assess the level of endorsement based on the content of the presented lectures. The following 4 topics (Figure 1) were presented to solicit an endorsement rating from 1 to 5:
“Uniportal Transforaminal Discectomy/Foraminotomy,” presented by Peter Derman, MD, Texas Back Institute, USA.
“Transforaminal Full-Endoscopic Interbody Fusion for Hard Disc Herniation,” presented by Zhen-Zhou Li, MD, Department of Orthopedics, Chinese PLA General Hospital, Beijing, China.
“Endoscopic Standalone Lumbar Interbody Fusion,” presented by Alvaro Dowling, MD, Endoscopic Spine Clinic, Santiago, Chile, Department of Orthopedic Surgery, USP, Ribeirão Preto, Brazil.
The Importance of Patient Feedback During Endoscopic Spine Surgery,” presented by Martin Knight, MD, Manchester University, The Spinal Foundation, London, UK.

Webinar moderator (Kai-Uwe Lewandrowski, MD) and presenters who presented on the following topics: (1) Peter Derman, MD, Texas Back Institute—”Uniportal Transforaminal Discectomy/Foraminotomy“; (2) Zhen-Zhou Li, MD, Department of Orthopedics, Chinese PLA General Hospital, Beijing, China—”Transforaminal Full-Endoscopic Interbody Fusion for Hard Disc Herniation”; (3) Alvaro Dowling, MD, Endoscopic Spine Clinic, Santiago, Chile—”Endoscopic Standalone Lumbar Interbody Fusion”; and (4) Martin Knight, MD, Manchester University, The Spinal Foundation, London, UK—”The Importance of Patient Feedback During Endoscopic Spine Surgery.”
Additionally, surgeons were asked to provide details about their postgraduate education and experience with endoscopic procedures. The data were exported to Excel and then analyzed using IBM SPSS (version 29.0.2.0) and Jamovi (version 2.3) software. The analysis employed descriptive metrics to quantify replies and compute averages, ranges, deviations, and percentages. The χ 2 test gauged the correlation between variables. A P value below 0.05 was deemed significant, with a 95% confidence interval applied to all statistical evaluations.
The Rasch Methodology
The authors employed the polytomous Rasch model analysis described by Andrich.6 When employed in a specific empirical scenario, this model posits that the likelihood of a certain result is a probabilistic outcome driven by these individual and item characteristics. Ordered response data incorporate the likelihood of an answer falling into a specific category (for instance, the chance of choosing strongly agree, agree, disagree, or strongly disagree). In the polytomous Rasch model, a score of x on a given item implies that an individual has simultaneously surpassed x thresholds below a certain region on the continuum and failed to surpass the remaining m – x thresholds above that region. In mathematical terms, the Rasch model application in the authors’ study represents the log odds (or logit) of a person endorsing an item as the difference between the person’s ability or level of partial agreement and the item’s difficulty. This model employs χ 2 fit statistics to control the applicability of data to the model. The χ 2 in common use is known as outfit and infit. These are reported as mean-squares, χ 2 statistics divided by their degrees of freedom, so they have a ratio-scale form with expectation 1 and range 0 to + infinity. In this study, the authors’ used the outfit statistics which is based on the conventional sum of squared standardized residuals, where X is an observation, E is its expected value based on Rasch parameter estimates, and σ² is its modeled variance about its expectation. Fit statistics are formulated to test particular hypotheses. The model’s fit with individual items was assessed through the item log residual fit statistics, the item-trait interaction fit test (using a χ 2 method). Decisions regarding fit compatibility were based on the collective outcomes of these methods. An item with a negative fit residual overdiscriminates compared with the overall set, while a positive value means it discriminates less effectively. Typically, a log residual fit statistic between −2.5 and 2.5 is considered acceptable.9 Therefore, outfit is dominated by unexpected outlying, off-target, low information responses and therefore is outlier-sensitive. The mean-square fit statistics show the size of the randomness (ie, the amount of distortion of the measurement system). Mean squares are always positive, and 1.0 is their expected value. Values less than 1.0 indicate that observations are too predictable (redundancy, data overfit the model). Values greater than 1.0 indicate unpredictability (unmodeled noise, data underfit the model). Outfit data between 0.6 and 1.4 indicate good fit of the Rasch model. Outside these parameters, confounding factors are likely.
Wright Plot, Category Probability Curves, and Person-Item Map Analysis
In this study, the compatibility of individual items with the model was assessed through (1) analysis of individual item log residual fit statistics, (2) the item-trait interaction fit test (utilizing a χ 2 method), (3) Wright plots, (4) the person-item maps, and (5) the category probability curve (CPC). The Wright plot serves as a visual tool designed to juxtapose item difficulty and a person’s ability on a standard scale by aligning items and respondents along a vertical logit scale, where logits are a unit of measurement that expresses the log odds of a person successfully or favorably responding to an item, reflecting the relative difficulty of items and the relative ability of persons.10 On this scale, items are placed on the left side, and person abilities are on the right. The higher up on the scale an item is placed, the more difficult it is considered to be. Conversely, individuals placed higher on the scale possess greater ability or trait levels relevant to the measured items. Additionally, Wright plots show whether the items appropriately target the abilities of the responding surgeons. For example, suppose most items cluster at the high end of the scale, but the person’s abilities are distributed toward the lower end. In that case, this mismatch suggests the test is too difficult for the surgeons participating in the webinar to agree or endorse the presented topic.
The person-item map visually represents the distribution of person abilities and item difficulties on a common scale.11 This map assesses the match between responding surgeons’ abilities (or attitudes, perceptions, level of endorsement, etc) and the characteristics of tasks or items (presented clinical evidence on 1 of the 4 topics). The person-item map places both surgeons and the webinar topics (eg, items, examination questions, and survey statements) on the same logit scale, a logarithmic scale of odds probabilities. The left side of the map typically displays the distribution of person abilities, with higher abilities toward the top and lower abilities toward the bottom. The right side of the map shows the items ranked by difficulty, with harder items placed higher and easier items placed lower. The person-item map facilitates a deeper understanding of how well the topic presented during the webinar effectively captured what responding surgeons thought of it and whether the test effectively covers the range of endorsement in the constructs of interest. The collective outcomes of these methods informed the determination of whether items properly conformed to or deviated from the model. A negative fit residual signifies that an item discriminates more than the average discrimination across all items, while a positive value indicates subpar discrimination. Typically, log residual fit statistics falling between –2.5 and 2.5 are deemed acceptable. The χ 2 test hypothesizes no discrepancy between observed and expected values for a specific item category. Consequently, P values below 0.05, denoting a discernible difference, signal an item’s inadequate conformity to the model. While x 2 values can differ and may escalate progressively when ordered, optimal conditions entail no abrupt surges and a lack of statistical significance.
In the CPC, the presentation of ordered response data integrates the probabilities associated with selecting certain response options, such as “strongly agree,” “agree,” “disagree,” or “strongly disagree.” It graphically represents how the likelihood of choosing a specific response option correlates with the respondent’s agreement level, applying this methodology across all categories. This curve plots the respondent’s position in terms of logits, which are the natural logarithm of the odds (on the x axis), indicating their agreement across various statements. As such, a respondent’s proclivity for agreeing with the evaluated attitudes pushes their logit position to the right, demonstrating a higher likelihood of favorably affirming the items. Consequently, the CPC effectively demonstrates how the probability of selecting a particular response option varies with the respondent’s agreement level and the question’s intensity or challenge. Our research showcases the CPCs across 4 items, each with 5 potential responses. In this context, ascending scores reflect an increased agreement with the statement or item at hand. “Ability” in our study measures how strongly a surgeon agrees with a question, whereas “item difficulty” assesses how straightforward it is to endorse the item. The point at which 2 adjacent categories’ CPCs intersect, indicating equal selection probability, is termed the threshold. For adherence to the Rasch model, these thresholds must follow a specific order, signifying that a choice of “strongly agree” reflects a deeper connection with the attribute than simply “agree.” Thus, surgeons possessing a higher level of the specific trait tend to choose more affirmative responses, while those with lower trait levels typically opt for less affirmative options.
RESULTS
Of the 1311 surgeons online at the beginning of the webinar, 76 accessed the prewebinar survey, 54 started it, and 42 submitted a complete survey resulting in a completion rate of 77.8% and an average time to complete of 53 seconds. The respondents were orthopedic surgeons (42.9%), neurosurgeons (31.0%), fellows (9.5%), and residents (7.1%). The mean professional experience (years in practice) was 12.74 (range, 1 to 33 years). Over 50% of responding surgeons had more than 15 years of practice. The postwebinar demographics were similar, with orthopedic surgeons (38.1%) comprising the largest group followed by neurosurgeons (33.3%), fellows (2.4%), and residents (2.4%). The mean years in practice was 16.64 (range, 1 to 40 years). The polytomous Rasch analysis conducted on the responses from participants of the ISASS webinar series on endoscopic spine surgery provided insightful data on endorsing various endoscopic procedures before and after the webinar. The items analyzed included the following:
uniportal transforaminal discectomy/foraminotomy
transforaminal full-endoscopic interbody fusion for hard disc herniation
endoscopic standalone lumbar interbody fusion
incorporation of patient feedback during surgery
Endorsement Shifts
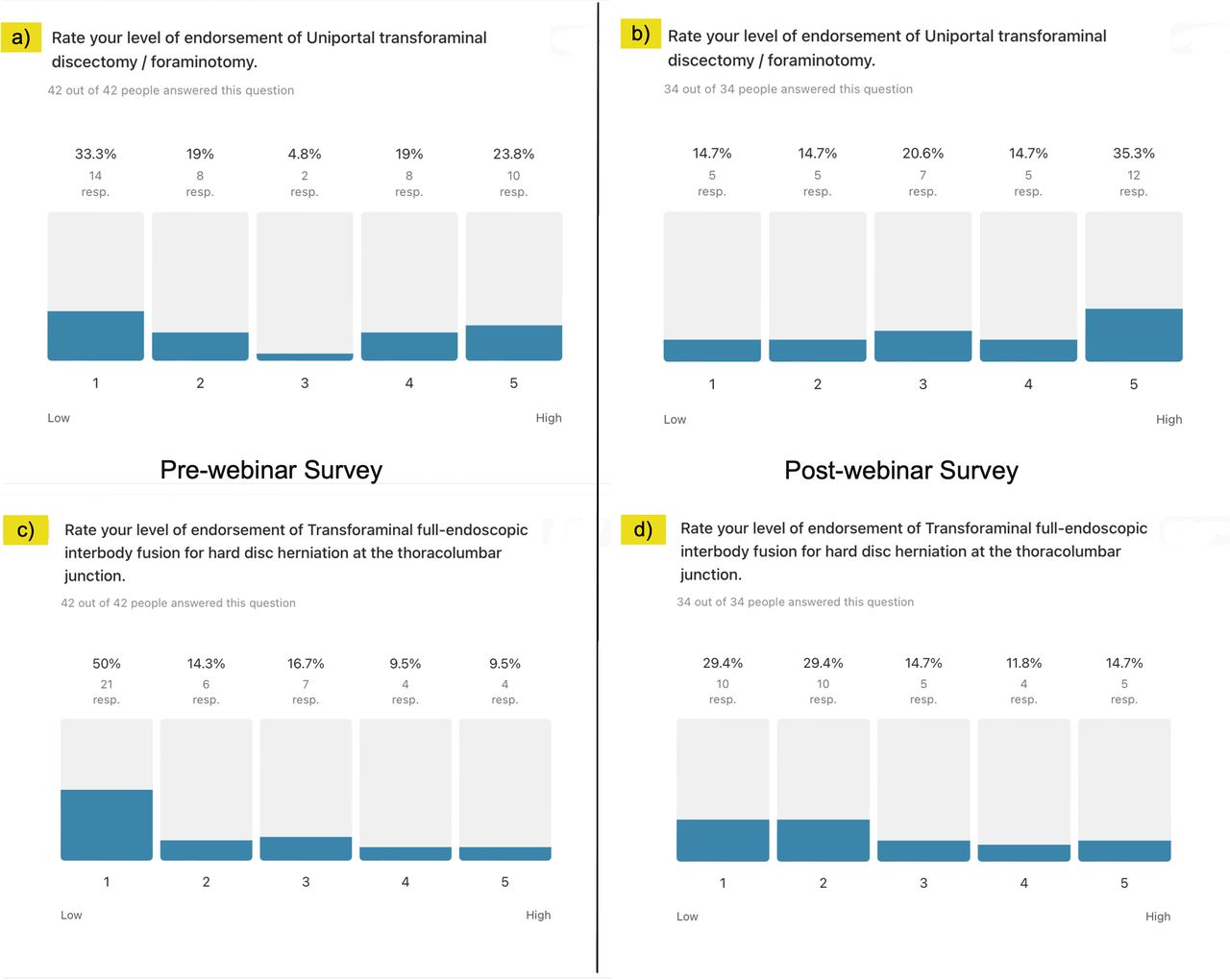
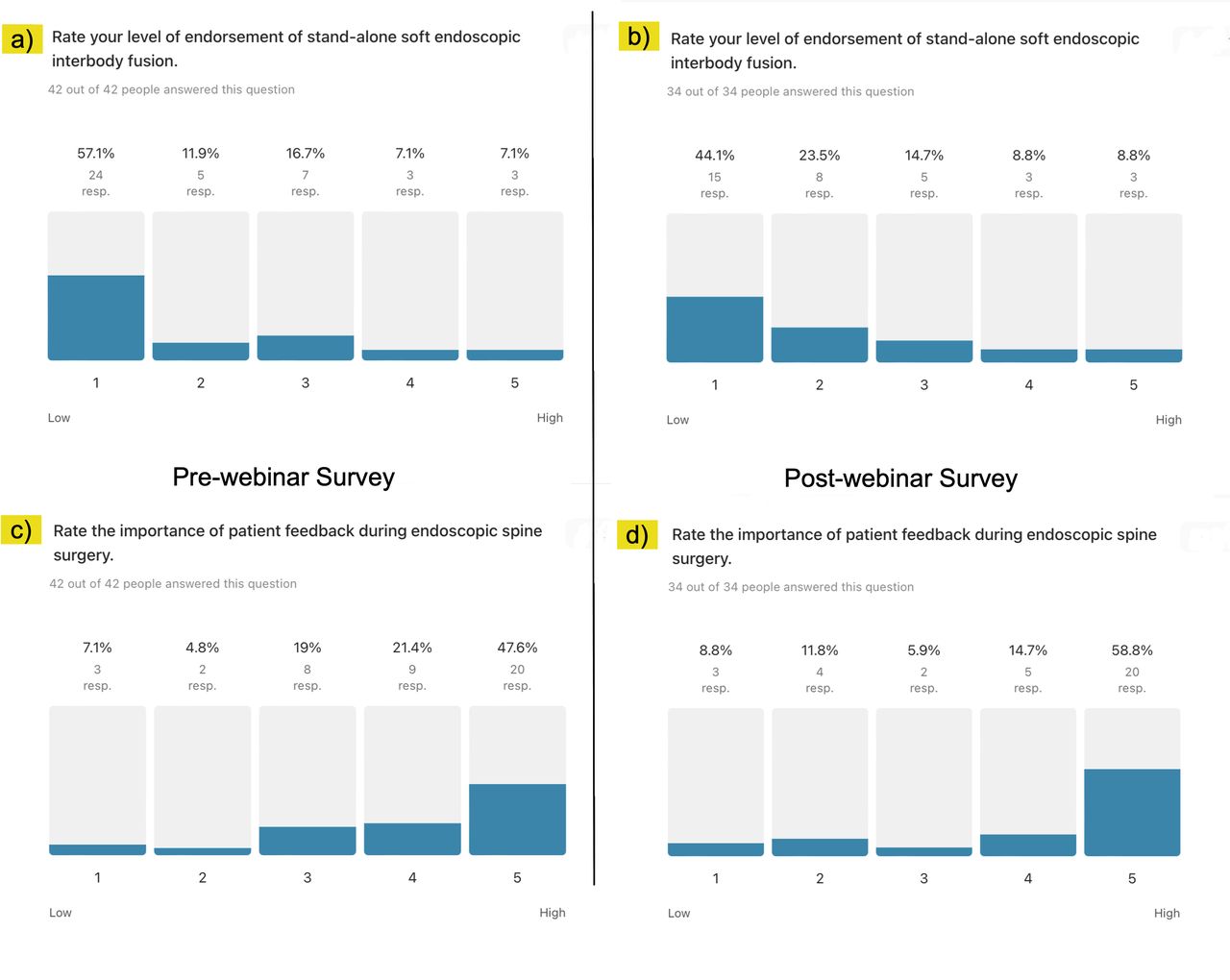
Descriptive statistics revealed a noticeable shift in participants’ confidence levels regarding the discussed procedures. Initially, 33.3% of participants expressed low confidence in the uniportal transforaminal discectomy/foraminotomy technique, which slightly decreased postwebinar, with 35.3% showcasing high confidence. Similarly, confidence in transforaminal full-endoscopic interbody fusion for hard disc herniation showed significant improvement, with low confidence levels dropping from 50.0% to 29.4% after the webinar (Figure 2). The level of endorsement for the endoscopic standalone lumbar interbody fusion experienced a reduction in low confidence from 57.1% to 44.1%. Moreover, high confidence in the importance of patient feedback during surgery increased from 47.8% to 58.3%, indicating a positive impact of the webinar on participants’ perceptions (Figure 3).

Descriptive statistics of level of endorsement analysis of endoscopic procedures. Regarding confidence in the uniportal transforaminal discectomy/foraminotomy technique, (a) 33.3% of participants had low confidence before the webinar and (b) 35.3% had high confidence after the webinar. Regarding confidence in the transforaminal full-endoscopic interbody fusion for hard disc herniation, (c) 50.0% had low confidence before the webinar and (d) 29.4% had low confidence after the webinar. The descriptive statistical analysis exposed the controversy surrounding the transforaminal full-endoscopic interbody fusion for hard disc herniation.

Descriptive statistics of level of endorsement analysis of endoscopic procedures. For endoscopic standalone lumbar interbody fusion, (a) 57.1% of participants had low confidence before the webinar (b) 44.1% had low confidence after the webinar. Regarding the need for patient feedback during endoscopic spine surgery, (c) 47.8% had high confidence before the webinar and (d) 58.3% had high confidence after the webinar. The descriptive statistical analysis exposed the controversy surrounding the endoscopic standalone lumbar interbody fusion.
Wright Plot, CPCs, and Person-Item Map Analysis
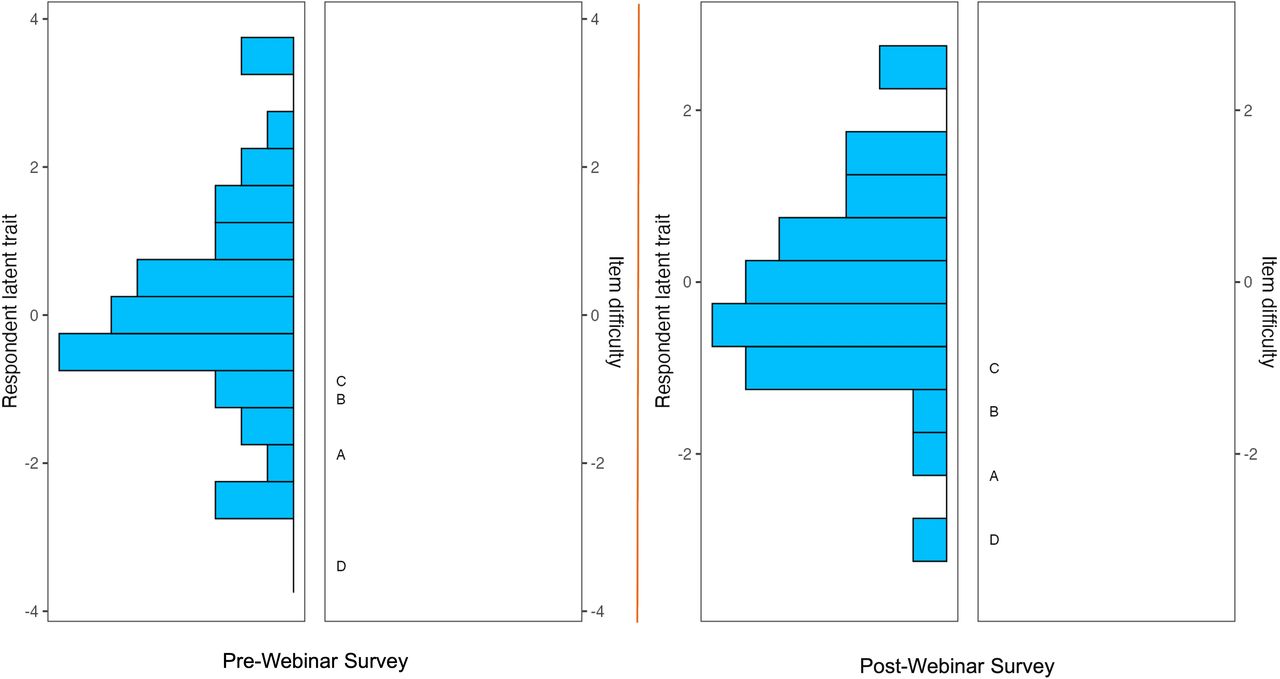
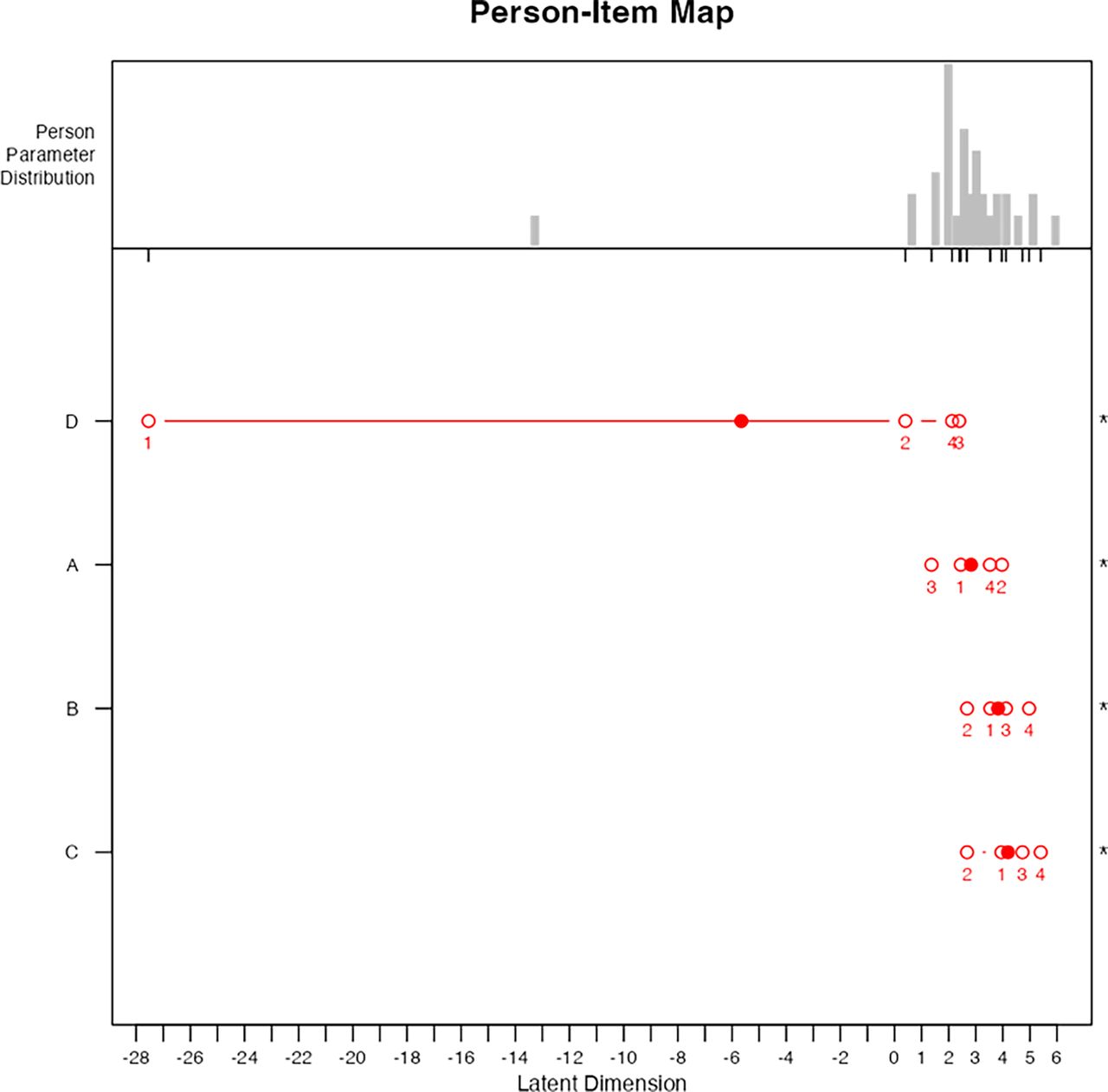
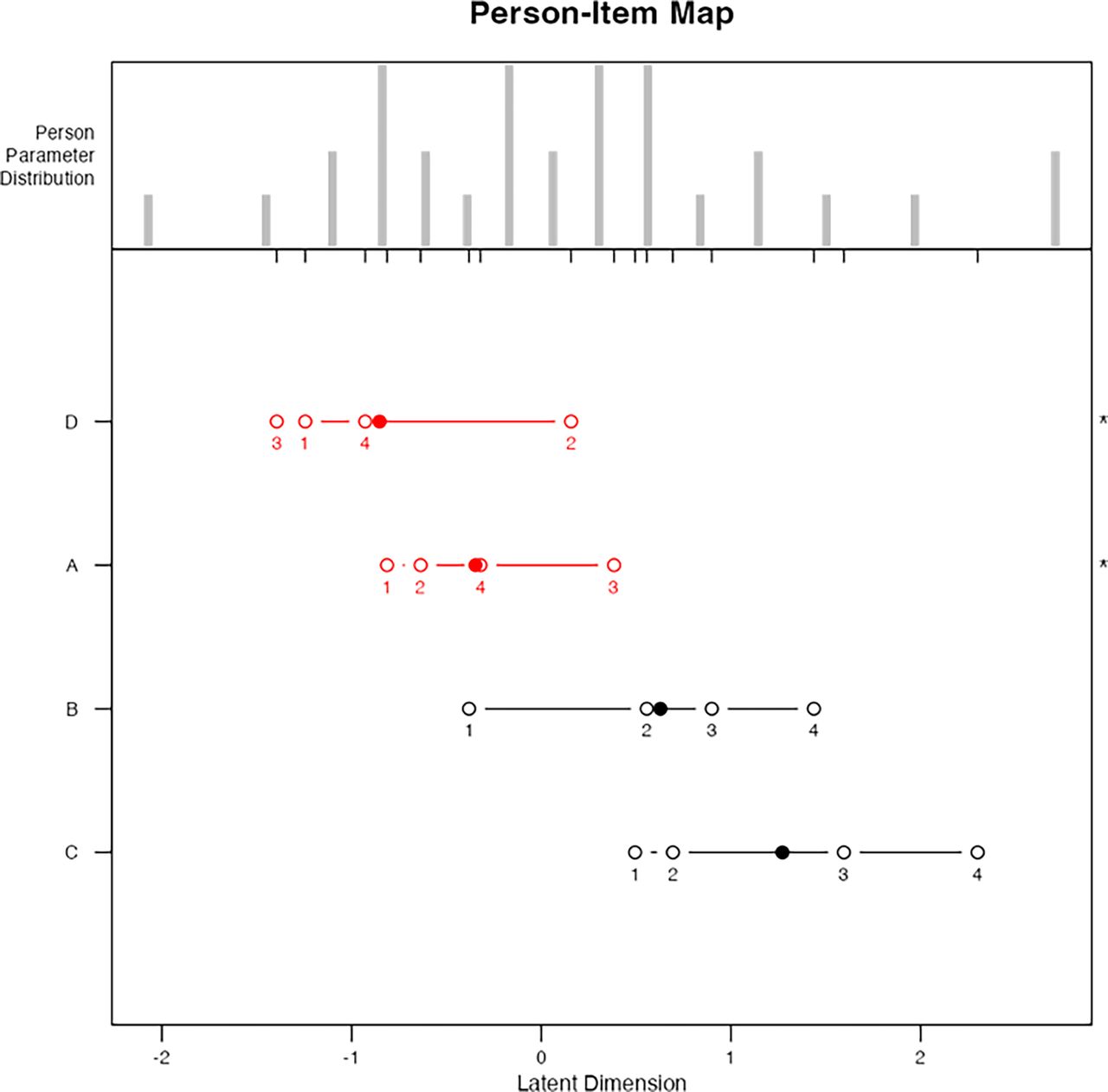
The Wright plot analysis before and after the webinar illustrated a clear distribution of surgeons’ endorsements across the discussed items. Surgeons with higher logits were more inclined to endorse the procedures positively, indicating a higher level of agreement or confidence in the techniques. Notably, the postwebinar Wright plot showed a more favorable endorsement for transforaminal full-endoscopic interbody fusion and endoscopic standalone lumbar interbody fusion, which were positioned toward the right, suggesting increased agreement among surgeons (Figure 4). The person-item map further details the distribution of endorsements and reveals the logistic transformation of person and item positions. The prewebinar map highlighted patient feedback during endoscopic spine surgery as the most challenging item for agreement, reflected by its mean logit location shifted to the left (Figure 5). Postwebinar responses indicated a significant reordering of item difficulty, with uniportal transforaminal discectomy/foraminotomy and patient feedback during endoscopic spine surgery, presenting disordered thresholds, suggesting issues in response category discrimination, or confounding factors not captured by the survey (Figure 6).

Wright plot obtained in the polytomous Rasch analysis of prewebinar (left panel) and postwebinar (right panel) survey responses. The item response theory polytomous Rasch partial agreement analysis was employed to assess spine surgeons’ level of endorsement of the 4 procedures (test items) presented during the webinar: (a) uniportal transforaminal discectomy/foraminotomy, (b) transforaminal full-endoscopic interbody fusion for hard disc herniation, (c) endoscopic standalone lumbar interbody fusion, and (d) patient feedback during endoscopic spine surgery. On the left side of the Wright plot, the responding surgeons’ latent traits are written in logits (log odds) as estimates of true intervals of item difficulty and surgeon ability. The surgeons represented by horizontal bars at the top indicated a higher level of endorsement for the individual test components of endoscopic spinal surgery (positive logits) than those on the bottom (negative logits). On the right, the higher-level endorsement items are listed at the top vs the more controversial ones on the bottom. Directly across from 0, those surgeons had a 50% chance of endorsing a test item. One logit above suggests an approximately 25% chance that the test item was endorsed vs 1 logit below suggests an approximately 75% chance of endorsement. There were no assessment gaps, suggesting there was no redundancy between test items.

The person-item map of prewebinar survey responses shows the logarithmically transformed person and item positions on a unified continuum using the logit measurement unit, transitioning ordinal data to equal-interval data. This method charts both person and item positions (in logits) along the x axis. Within Rasch modeling, these values are labeled as “locations” rather than “scores.” A surgeon’s logit location indicates their natural log odds of agreement with a series of items. Individuals with pronounced adherence to the considered attitude affirm items favorably, positioning them further to the right on the scale. The solid dots indicate the mean person location scores. Contrary to the descriptive statistical analysis (Figure 2), the most challenging item to agree on was item D “patient feedback during endoscopic spine surgery” with the mean logit location (1) shifted to the left. The mean logit location for item A (uniportal transforaminal discectomy/foraminotomy), item B (transforaminal full-endoscopic interbody fusion for hard disc herniation), and item C (endoscopic standalone lumbar interbody fusion) were more shifted to the right of the plot, therefore showing more intense partial agreement for these items. The person-item maps also illustrate that items were reasonably well distributed. However, some surgeons could not be measured as reliably as the majority by this set of items, indicating the test items were either too intense or not intense enough for them (item D; logit location 1 to the left). The analysis also showed disordered thresholds of endorsement for the 4 test items, suggesting that surgeons had difficulty consistently discriminating between response categories ranging from strongly disagree, disagree, agree, to strongly agree—a problem observed when there are too many response options not measuring the opinions. All 4 of the item topics before being presented during the webinar were disordered and are shown in red. Examining the order and location of these test items reveals an uneven distribution of the ranked order of item difficulties or intensities along the logit continuum, suggesting a poor fit to the Rasch model with statistically significant difference between the observed values and the values predicted by the model.

The person-item map of postwebinar survey responses shows the logarithmically transformed person and item positions on a unified continuum using the logit measurement unit, transitioning ordinal data to equal-interval data. This method charts both person and item positions (in logits) along the x-axis. Within Rasch modeling, these values are labeled as “locations” rather than “scores.” A surgeon’s logit location indicates their natural log odds of agreement with a series of items. Individuals with pronounced adherence to the considered attitude affirm items favorably, positioning them further to the right on the scale. The solid dots indicate the mean person location scores. Contrary to the descriptive statistical analysis (Figure 3), after the webinar, the most challenging item to agree on was still item D, patient feedback during endoscopic spine surgery, with the mean logit location being out of order (3, 1, 4, and 2) and item A (uniportal transforaminal discectomy/foraminotomy) with the mean logit location also out of order (1, 2, 4, and 3), suggesting that surgeons had difficulty consistently discriminating between response categories—a problem observed when there are too many response options not measuring the opinions. Examining the order and location of these test items reveals an uneven distribution of the ranked order of item difficulties or intensities along the logit continuum suggesting a poor fit to the Rasch model with statistically significant difference between the observed values and the values predicted by the model. Contrary to the descriptive statistics, which suggested item B (transforaminal full-endoscopic interbody fusion for hard disc herniation) and item C (endoscopic standalone lumbar interbody fusion) were controversial, these items were shifted more to the right of the plot, therefore showing more intense partial agreement and endorsement for these items. The clinical evidence presented in these item presentations during the webinar was more convincing to the webinar participants. The person-item maps on top of the graph also illustrate that items were reasonably well distributed.
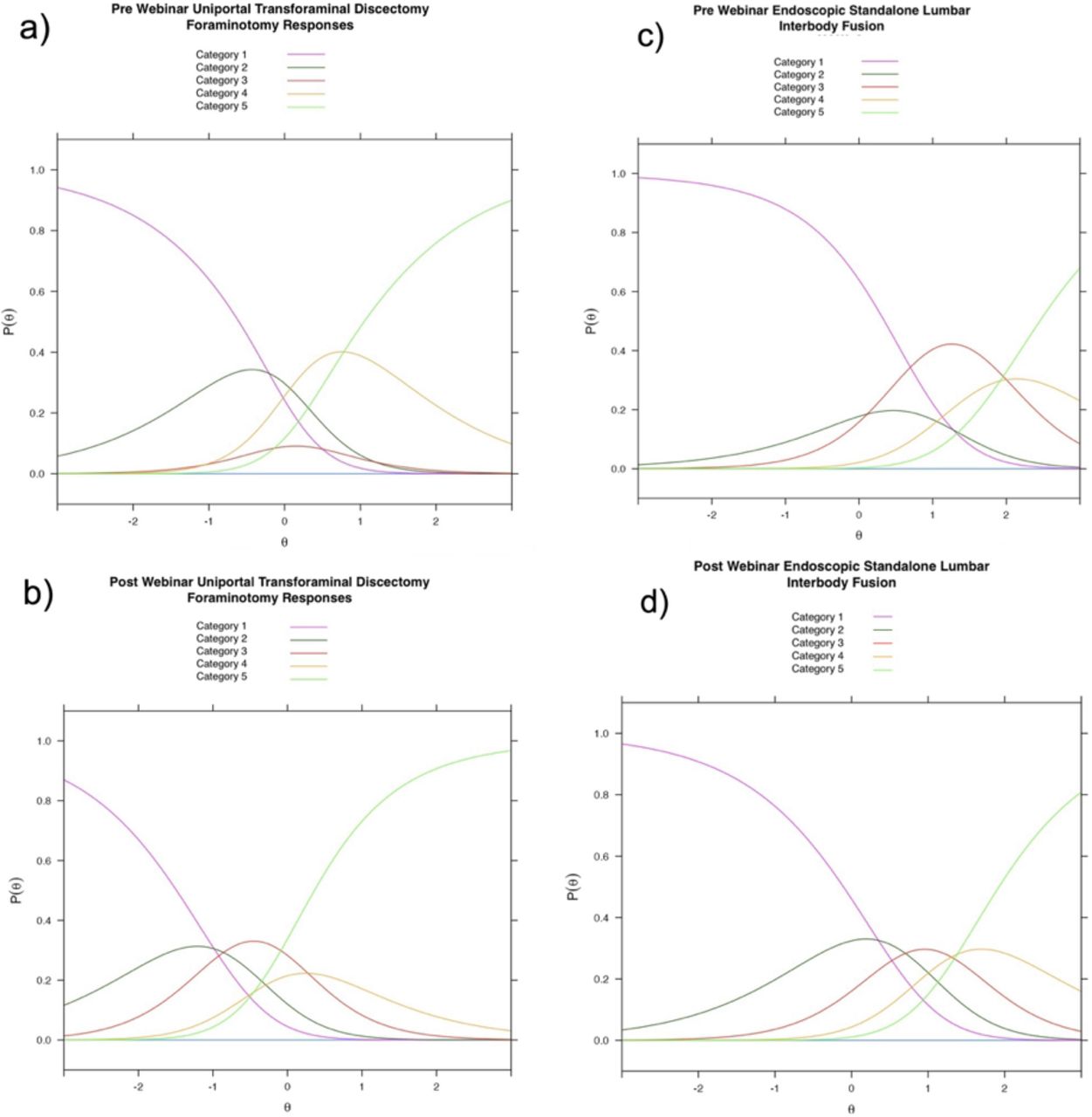
The CPC corroborated these findings. After the webinar, disordered sequencing was converted to ordered sequencing of the thresholds (crossover between CPCs of 2 neighboring categories having an equal likelihood of selection; Figure 7), which were graphically demonstrated for the endoscopic standalone lumbar interbody fusion and transforaminal full-endoscopic interbody fusion for hard disc herniation. As a result of what participants learned during the webinar about the endoscopic standalone fusion technique and its associated clinical outcomes, response data conformed to the Rasch model, suggesting endorsement without significant confounding factors. The response threshold sequencing remained disordered for the uniportal transforaminal discectomy/foraminotomy and patient feedback during endoscopic spine surgery, suggesting that for surgeons located anywhere along the response continuum, and especially for those surgeons located at the maximum value for this category, disagreeing with the item (ie, selecting category strongly disagree) is never the most probable response. Confounding factors not captured by the survey were likely present.

Category probability curves (CPCs) are shown for test items uniportal transforaminal discectomy/foraminotomy and endoscopic standalone lumbar interbody fusion. They visually depict the relationship between the probability of a particular category being chosen and the respondent surgeon’s stance generated for each category. After the webinar, disordered sequencing was converted to ordered sequencing of the thresholds (crossover between CPCs of 2 neighboring categories having an equal likelihood of selection), which were graphically demonstrated for the endoscopic standalone lumbar interbody fusion. As a result of what participants learned during the webinar about the endoscopic standalone fusion technique and its associated clinical outcomes, response data conformed to the Rasch model, suggesting endorsement without significant confounding factors. However, the portion of surgeons with low confidence in this procedure (Category 1) and who could not be convinced otherwise remained the same. The response threshold sequencing remained disordered for uniportal transforaminal discectomy/foraminotomy, suggesting that for surgeons located anywhere along the response continuum, and especially for those surgeons located at the maximum value for this category, disagreeing with the item (ie, selecting category strongly disagree) is never the most probable response. Confounding factors not captured by the survey were likely present.
Outfit Analysis
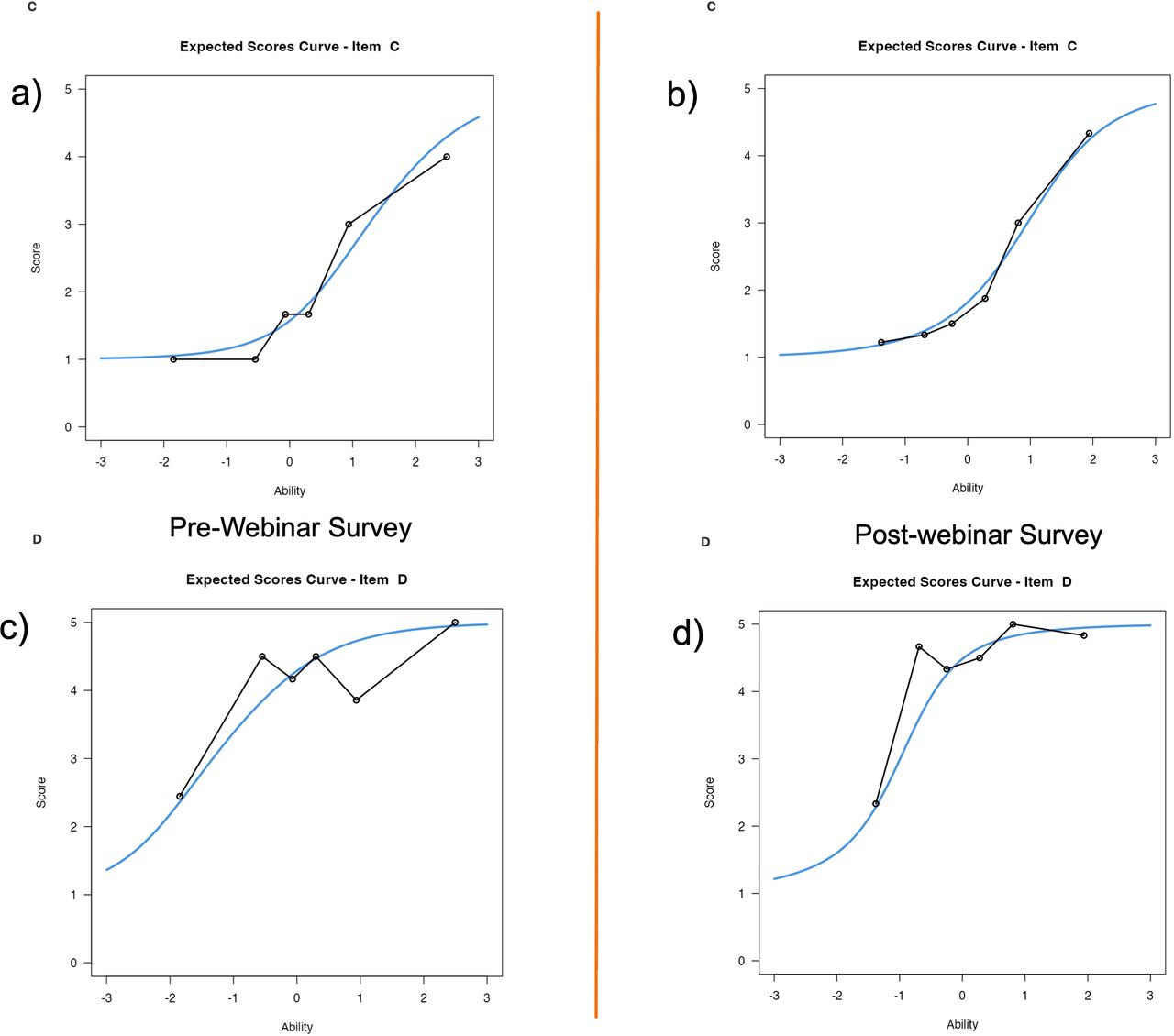
Outfit mean-square statistics provided insight into the model fit for each item. Prewebinar responses to uniportal transforaminal discectomy/foraminotomy showed an outfit of 0.840, which increased to 1.042 postwebinar, indicating unresolved confounding factors and slightly underfitting the predictions by the Rasch model. The outfit analysis for transforaminal full-endoscopic interbody fusion for hard disc herniation showed improved outfit after the webinar by increasing from 0.532 prewebinar to 0.727 postwebinar. Postwebinar responses fit the Rasch model better (Figure 8). Conversely, the endoscopic standalone lumbar interbody fusion improved model fit postwebinar, with outfit values moving from 0.721 prewebinar closer to the ideal range of 0.6 to 1.4 with a postwebinar outfit of 0.793 but still overfitting the Rasch model. The patient feedback during endoscopic spine surgery analysis demonstrated an improved fit to the Rasch model with the outfit decreasing from 1.878 prewebinar to 1.390 postwebinar. While still underfitting the model with some unpredictable answers remaining, these calculations suggest that the webinar presentations effectively addressed previous confounding factors and resolved some controversial issues to affect improved model fit (Figure 9).

Two examples of outlier-sensitive means statistics (outfit analysis) based on the conventional sum of squared standardized residuals, which is more sensitive to unexpected observations, are shown. Surgeon prewebinar (a and c) compared with postwebinar (b and d) endorsement responses showed greater outfit (0.840 prewebinar vs 1.042 postwebinar) from the model predicted by the Rasch analysis for item A (uniportal transforaminal discectomy/foraminotomy) after the webinar, suggesting the presence of confounding factors affecting responses on item A that were not convincingly resolved in the presentation. The outfit analysis for item B (transforaminal full-endoscopic interbody fusion for hard disc herniation) showed greater outfit (0.532 prewebinar vs 0.727 postwebinar) after the webinar as well. Postwebinar responses fit the Rasch model well. Outfit data between 0.6 and 1.4 indicate good fit of the Rasch model.

Two examples of outlier-sensitive means statistics (outfit analysis) based on the conventional sum of squared standardized residuals, which is more sensitive to unexpected observations, are shown. Surgeon prewebinar (a and c) compared with postwebinar (b and d) endorsement responses showed similar outfit (0.721 prewebinar vs 0.793 postwebinar) from the model and better graphic fit predicted by the Rasch analysis for item C (endoscopic standalone lumbar interbody fusion) after the webinar, suggesting that the presentation was able to resolve many confounding factors affecting responses on item C. The outfit analysis for item D (patient feedback during endoscopic spine surgery) showed lesser outfit (1.878 prewebinar vs 1.390 postwebinar) after the webinar, indicating that the presentation on item D was convincing and resulted in responses that followed the Rasch model better. Outfit data between 0.6 and 1.4 indicate good fit of the Rasch model.
DISCUSSION
The first of 4 ISASS webinars on current and emerging techniques in endoscopic spine surgery has significantly influenced the perceptions and endorsements of spine surgeons regarding several endoscopic procedures. Utilizing the polytomous Rasch model for analyzing surgeon endorsements has provided a unique insight into how education and exposure to advanced techniques can shift professional confidence and acceptance of innovative surgical approaches.
The Rasch’s analysis Wright plot (Figure 4) and person-item map analyses (Figures 5 and 6) further aided in the interpretation of surgeon endorsements, offering a visual representation of changes in perception before and after the webinar. These analyses demonstrated that the webinar series successfully targeted areas of initial low confidence among surgeons, translating into higher endorsement levels postwebinar. The shift in logits in the Wright plot postwebinar, particularly for the transforaminal full-endoscopic interbody fusion and endoscopic standalone lumbar interbody fusion, indicates a collective movement toward a more favorable view of these techniques.
The outfit analysis highlighted the nuanced impact of the webinar on surgeon endorsements, with some procedures showing significant changes in model fit statistics postwebinar (Figures 7 and 8). These changes suggest that the webinar speakers effectively addressed specific confounding factors and ambiguities that previously influenced surgeons’ perceptions of particular techniques. The out-of-order person-item plots on uniportal transforaminal discectomy/foraminotomy12 and patient feedback during endoscopic spine surgery13 after the webinar could point to ongoing controversies surrounding these topics but more likely are related to a lower level of curiosity on these more accepted issues.14–20
The data revealed notable shifts in surgeons’ confidence levels, particularly for the clinical evidence presented on the transforaminal instrumented interbody fusion across the thoracolumbar junction21 and standalone lumbar interbody fusion techniques,22 with improvement observed in the endorsement of transforaminal full-endoscopic interbody fusion for hard disc herniation and the endoscopic standalone lumbar interbody fusion after the webinar. The survey showed significant controversy on these endoscopic fusion topics with lower endorsement levels demonstrated by the prewebinar responses (Figures 2 and 3). The standalone technique employed a corticocancellous bone allograft enriched with platelet-rich plasma and mesenchymal stem cells. These 2 techniques were initially met with the highest level of skepticism. In the postwebinar survey, higher endorsement levels were noted in the CPCs, as responses shifted from categories 2 and 3 to categories 4 and 5 with ordered thresholds. This shift signifies the speakers’ effectiveness in not only presenting these 2 fusion techniques and the associated clinical outcomes convincingly, but it may also represent the responding surgeons’ higher interest level in these novel cutting-edge endoscopic fusion surgeries in comparison to the more bread-and-butter issues of foraminal decompression and awake surgery. Nevertheless, each of the 4 topics garnered elevated confidence ratings, underscoring the webinar’s efficacy in enriching spine surgeon education and illuminating evolving trends in spine surgery, thus warranting endorsement by spine societies through policy formulation and coverage statements to ensure adequate reimbursement, along with the refinement of clinical guidelines.
CONCLUSIONS
The application of the polytomous Rasch model in the analysis of participating surgeons’ responses has provided a comprehensive understanding of the impact of educational interventions on professional perceptions and endorsements for 4 endoscopic spinal surgery protocols. The descriptive statistics suggested the lowest endorsement level for endoscopic fusion procedures. However, the Rasch analysis showed an ordered endorsement shift at the end of the webinar, suggesting that endoscopic spinal fusion is considered a surgical technique relevant to most spine surgeons. Knowledge gaps, webinar participants’ disinterest for the tried-and-true, and their adherence to preconceived notions of clinical outcomes with competing alternative surgical techniques are likely to be blamed for the lower level of endorsement for the transforaminal discectomy/foraminotomy technique. Feedback-based endoscopic surgery treating validated pain generators remained less controversial at the end of the webinar but inconsistent level of endorsement as evidenced by disordered thresholds in the CPCs persisted. While there are likely many confounding factors and explanations not captured by the survey, this surgeon survey study clearly indicated a high level of interest in applying the endoscopic surgery platform with other advanced technologies such as minimally invasive fusion techniques with expandable cages and transpedicular fixation techniques.
Footnotes
↵† International Society for the Advancement of Spine Surgery, Interamerican Society for Minimally Invasive Spine Surgery - La Sociedad Interamericana de Cirugía de Columna Mínimamente Invasiva (SICCMI), International Intradisccal Therapy Society (IITS.org)
↵‡ Interamerican Society for Minimally Invasive Spine Surgery - La Sociedad Interamericana de Cirugía de Columna Mínimamente Invasiva (SICCMI)
↵§ Minimally Invasive Spine Surgery Section of the Chinese Orthopedic Association, International Society for Endoscopic Spine Surgery (ISESS)
↵¶ International Society for the Advancement of Spine Surgery, President
Funding ISASS received funding from Lange MedTech for the webinar and the publication of this special issue. Funding was paid directly to the organization. No formal funding by private, government, or commercial funders was received by the authors.
Declaration of Conflicting Interests The authors declare no conflict of interest relevant to this research, and there was no personal circumstance or interest that may be perceived as inappropriately influencing the representation or interpretation of reported research results. This research was not compiled to enrich anyone.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.