


Abstract
Background Biportal endoscopic transforaminal lumbar interbody fusion (BE-TLIF) is a minimally invasive TLIF (MIS-TLIF) technique, commonly performed with various cage types. Expandable cages are particularly effective in achieving segmental lordosis (SL) and disc height (DH) elevation in minimally invasive TLIF. However, the published literature lacks details regarding how these outcomes can be accomplished using BE-TLIF with an expandable cage.
Methods Nine cases (10 levels) of BE-TLIF with an expandable cage were reviewed. Procedures including unilateral laminotomy and bilateral decompression, cage expansion trials, and bilateral facetectomies were carried out under biportal endoscopy to achieve SL and DH elevation. Postoperative standing x-ray images at 3 months and reconstructed computed tomography images were analyzed. The sublaminar decompression angle—measured as the angle between the spinous process and the sublaminar decompression line on axial computed tomography—was used to evaluate contralateral sublaminar decompression.
Results All procedures were completed without changes to the surgical methods. Eight patients underwent single-level fusion, with 4 of them receiving additional decompression at adjacent levels. One patient underwent a 2-level fusion. Four cases utilized 12° lordotic cages, while the rest employed 20° hyperlordotic cages. The total time for each fusion was 152.5 ± 38.5 minutes. Segmental lordosis increased by 5.1°, with anterior and posterior DH elevations of 4.8 ± 1.7 mm and 3.1 ± 1.8 mm, respectively. No endplate injuries or early cage subsidence occurred. The mean sublaminar decompression angle was 31.8° ± 7.0°.
Conclusions BE-TLIF with an expandable cage may offer benefits in SL correction and DH elevation. These advantages are attributed to the use of more lordotic expandable cages, combined with contralateral facetectomies and careful endplate preparation—key features of the BE-TLIF technique.
Clinical Relevance SL correction and DH elevation can be achieved through BE-TLIF, which helps to reduce the recurrence of symptoms and improves the lumbar lordotic curve.
Level of Evidence 4.
- biportal endoscopic TLIF
- expandable cage
- biportal endoscopic spine surgery
- minimally invasive TLIF
- hyperlordotic expandable cages
Introduction
Lumbar interbody fusion is a surgical technique used to treat lumbar stenosis and instability between vertebral segments when nonsurgical options are ineffective. Achieving adequate segmental lordosis (SL) and disc height (DH) during fusion surgery is critical for successful outcomes.1 Among the various approaches to accessing the disc space, the posterior techniques, such as posterior lumbar interbody fusion and transforaminal lumbar interbody fusion (TLIF), allow for direct decompression of the central canal.2 However, since the cage is inserted posteriorly, achieving sufficient SL and DH elevation can be challenging.3 As a solution, expandable cages, which can adequately elevate the anterior DH after insertion, have been developed.4
Minimally invasive spine surgeries (MISS) have gained popularity due to the reduced invasiveness compared with traditional spine surgeries. Since the early 2000s, minimally invasive TLIF (MIS-TLIF), performed with microscopes and tubular retractors, has become a common practice.5,6 To achieve SL and DH elevation with smaller incisions and less muscle detachment, expandable cages have been introduced in MIS-TLIF procedures.7,8 However, there is ongoing debate about the effectiveness of expandable cages in MIS-TLIF. While some studies report improvements in radiographic parameters such as SL and DH,7–9 others have noted concerns about cage subsidence, questioning its long-term effectiveness.10
Biportal endoscopic spine surgery (BESS), a type of MISS, has gained popularity due to its familiarity for surgeons and ease of use. It offers a similar field of view to a microscope and allows for greater freedom of instrument movement through dual incisions.11 As more surgeons adopt unilateral laminotomy with bilateral decompression (ULBD) using BESS, the biportal endoscopic TLIF (BE-TLIF) has also emerged as a viable technique.12–14 BE-TLIF provides a similar surgical view to microscopic MIS-TLIF and allows for meticulous endplate preparation through direct visualization of the intervertebral space. Additionally, it facilitates direct decompression of the bilateral canal space using a 30° scope from a unilateral approach.15–18
Various cage types have been used during BE-TLIF, and the expandable cage is a promising option. Although some studies have reported on the surgical outcomes of BE-TLIF with expandable cages, no study has thoroughly described the procedure in detail, particularly regarding its potential to achieve SL and DH elevation.19,20
The purpose of this study is to review the procedure of BE-TLIF with an expandable cage at our hospital, analyze the outcomes with a focus on SL and DH elevation, and provide surgical tips to enhance the effectiveness of the procedure.
Methods
Research Ethics
As this was a retrospective case series study based on the review of patients’ medical records after surgery, consent to participate was exempted. The study was approved by the Institutional Review Board (IRB) at our hospital (30-2024-49, SMG-SNU BMC IRB).
Materials
This review included 9 patients (10 levels) who underwent BE-TLIF with expandable cages at our hospital between June 2023 and June 2024. The indications for BE-TLIF with an expandable cage are the same as those for conventional MIS-TLIF. Similarly, the absolute contraindications are identical to those of conventional MIS-TLIF.
Expandable Cage
We used Excender expandable cages (CG Bio, South Korea). These cages have a width of 11 mm and are available in 2 lengths: 28 and 32 mm. The cages offer fixed angles with 2 options: 12° (lordotic) and 20° (hyperlordotic). The initial cage height is either 8 or 10 mm, and it can be expanded by up to 4 mm using a torque driver. A trial implant is available to test the cage’s expansion capability. After the final cage insertion, additional bone grafts, such as hydroxyapatites or rhBMP2, can be injected through a posterior injection channel.
Surgical Procedure
The instruments used for BE-TLIF are the same as those employed in conventional BE-TLIF. At our hospital, arthroscopic devices (Arthrex, Florida, USA) and 30° scopes were used, along with radiofrequency ablators (Delphi, South Korea) for ablation and coagulation. Other instruments were standard for MIS-TLIF procedures.
All surgeries were performed under general anesthesia, with the patient positioned prone on a spine table. Standard skin preparation and draping were carried out. The approach direction was based on the side with the more severe radiating pain, although, due to the benefits of BESS in performing ULBD, a left-sided approach was generally preferred. The surgeon stood on the left side of the patient, while the devices, including arthroscopic tools and the C-arm, were positioned on the right side.
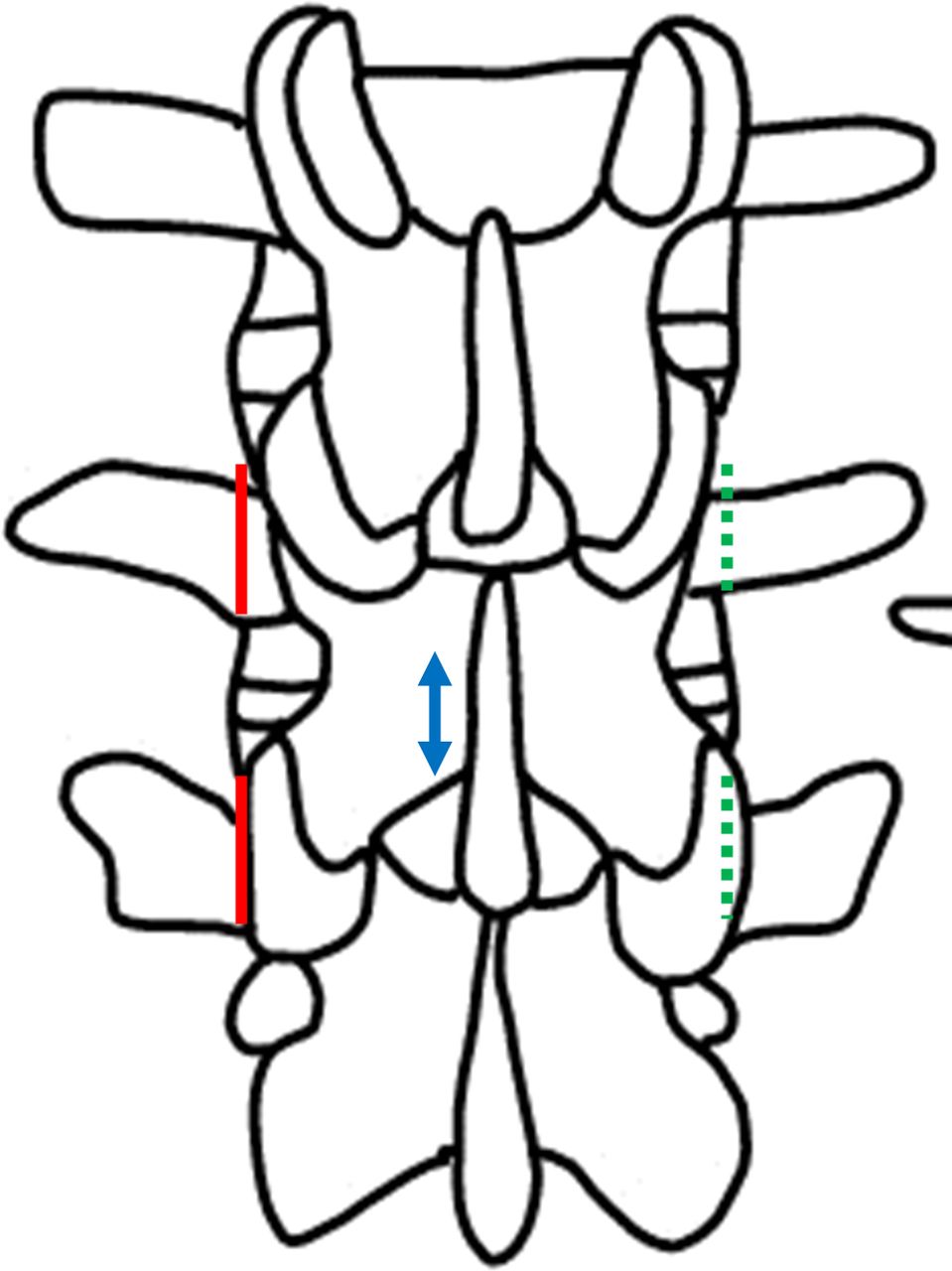
This procedure is a variation of the posterolateral trans-Kambin interlaminar TLIF. Three incisions are made as part of the process (Figure 1).

Incisions for biportal endoscopic transforaminal lumbar interbody fusion with an expandable cage. Red solid lines: 2 longitudinal 1-cm incisions lateral to the pedicle margin for biportal endoscopic procedures and percutaneous pedicle screw placement. These are referred to as the cranial and caudal biportal incisions. Blue arrow line: a less than 1 cm longitudinal incision just lateral to the midline, known as the quarterback incision. Green dotted lines: 2 longitudinal 1-cm incisions lateral to the pedicle margin for contralateral percutaneous pedicle screw insertions.
First, after identifying the midline and disc space via C-arm, 2 longitudinal 1-cm incisions are made lateral to the upper and lower lumbar pedicle margins. These incisions, commonly used for BE-TLIF and percutaneous pedicle screws, are referred to as cranial and caudal biportal incisions.11,13,21 Using these 2 incisions, the periosteal muscle detachment of the lamina and ipsilateral facet joint is performed with a periosteal elevator. After serial dilation using a tubular dilator to widen the fascia, a 30° scope is inserted through the cranial biportal incision. Saline, maintained at a pressure of 30 mmHg using a pressure-controlled arthroscopic pump, is used for fluid management.
A high-speed diamond burr is then employed to perform a unilateral laminotomy and resection of the deep portion of the interspinous ligament while preserving the superficial spinous process. Next, contralateral sublaminar bony resection is performed to achieve bilateral decompression, with complete resection of the ligamentum flavum (ULBD) until both traversing nerve roots are visualized and free. During this process, the 30° scope is rotated toward the contralateral side, providing a wide view of the epidural space beneath the midline. Once full decompression of the dura is confirmed, bilateral facetectomies are performed with reduced risk of neural tissue damage. This procedure includes total ipsilateral synovectomy, complete resection of the ipsilateral inferior articular process (IAP), partial resection of the ipsilateral superior articular process (SAP), partial contralateral synovectomy, and partial resection of both the contralateral IAP and SAP. The scope is first rotated toward the ipsilateral side to inspect the remaining facet joint after laminotomy. Using tools such as a chisel or osteotome, the remaining IAP and partial SAP are carefully removed to ensure sufficient space for smooth cage insertion without bony obstructions, as excessive resection of the SAP can lead to bleeding. The annulotomy and discectomy are then performed via the caudal biportal incision. The endplate preparation is continuously monitored through the cranial biportal portal with the endoscope.
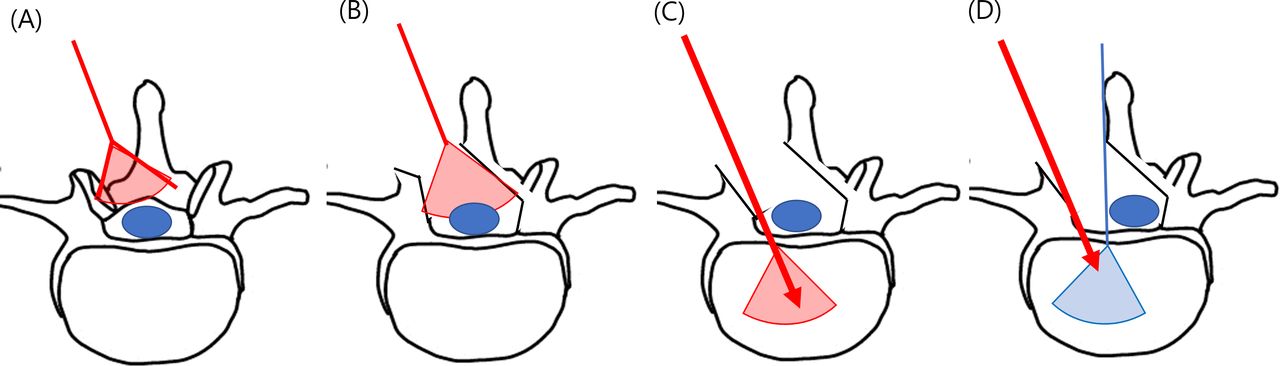
If necessary, an additional small incision, called the “quarterback incision,” can be made near the midline. This incision is less than 1 cm in size and allows for the insertion of additional instruments, such as root retractors. It can be used for additional endoscopic view, additional ipsilateral discectomy, dura retraction, and drain insertion (Figures 2 and 3).

(A) Covered field of view of the 30° scope before laminotomy. (B) Covered field of view of the 30° scope after unilateral laminotomy and bilateral decompression. (C) Red arrow indicates additional facetectomy, discectomy, and cage insertion. (D) Blue line marks the quarterback incision, which can be used for the endoscope, additional ipsilateral discectomy, dura retraction, and drain insertion.

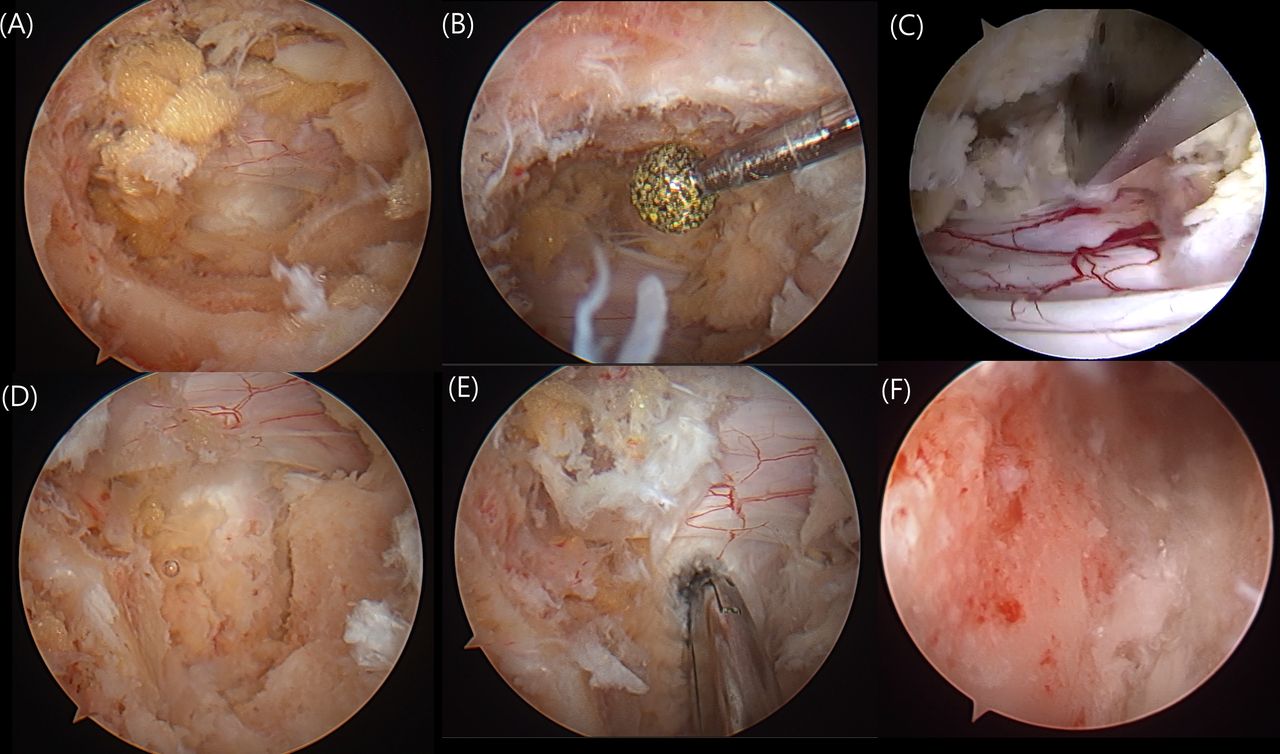
Endoscopic view. (A) Decompressed central canal after unilateral laminotomy. (B) Contralateral sublaminar bony resection while preserving the spinous process. (C) Contralateral sublaminar partial facetectomy performed using an osteotome. (D) After ipsilateral total inferior articular process and partial superior articular process resection. (E) Discectomy performed through the caudal biportal incision and quarterback incision. (F) Endoscope insertion into the disc space to inspect endplate preparation via the quarterback incision.
The cage trial is then inserted into the intervertebral space. After trial insertion, possible expansion is verified using the C-arm. If the expansion is insufficient, additional contralateral facetectomy is performed until adequate release between the 2 vertebral bodies is confirmed, which is checked again using the cage trial. Following this, the conventional BE-TLIF procedures are completed. Bone grafting is done via a funnel, using a mixture of autologous bone from the facetectomy and other bone substitutes.
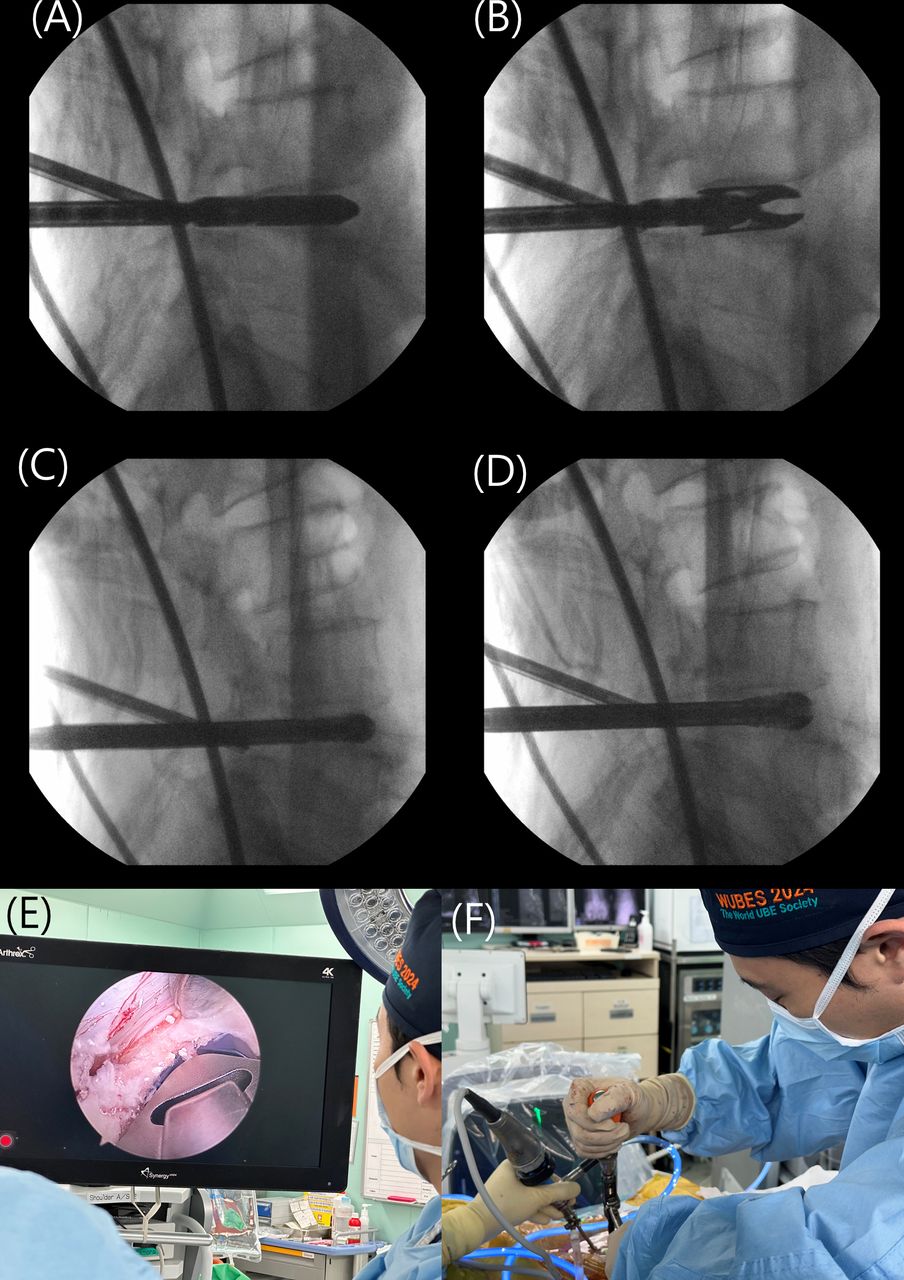
The real expandable cage is inserted via the caudal biportal incision from a lateral-to-medial and posterior-to-anterior direction to ensure it reaches the anterior epiphyseal ring, providing sufficient anterior positioning and epiphyseal ring support. During cage insertion, root retractors can be positioned via the quarterback incision to prevent dura injuries. Once the cage is fully expanded, additional bone grafts, such as rhBMP2, can be delivered through the posterior injection channel. Meticulous hemostasis is achieved, and a surgical drain can be placed via the quarterback incision. Percutaneous pedicle screw insertion and rod fixation are performed through the previous biportal endoscopy incisions and new contralateral percutaneous pedicle fixation incisions (Figure 4).

(A and B) C-arm images showing the cage expansion trial. (C and D) C-arm images of the real cage insertion and expansion. (E) Real cage insertion with dura protection using a root retractor via the quarterback incision. (F) Real cage expansion using a torque driver.
Outcome Measurements
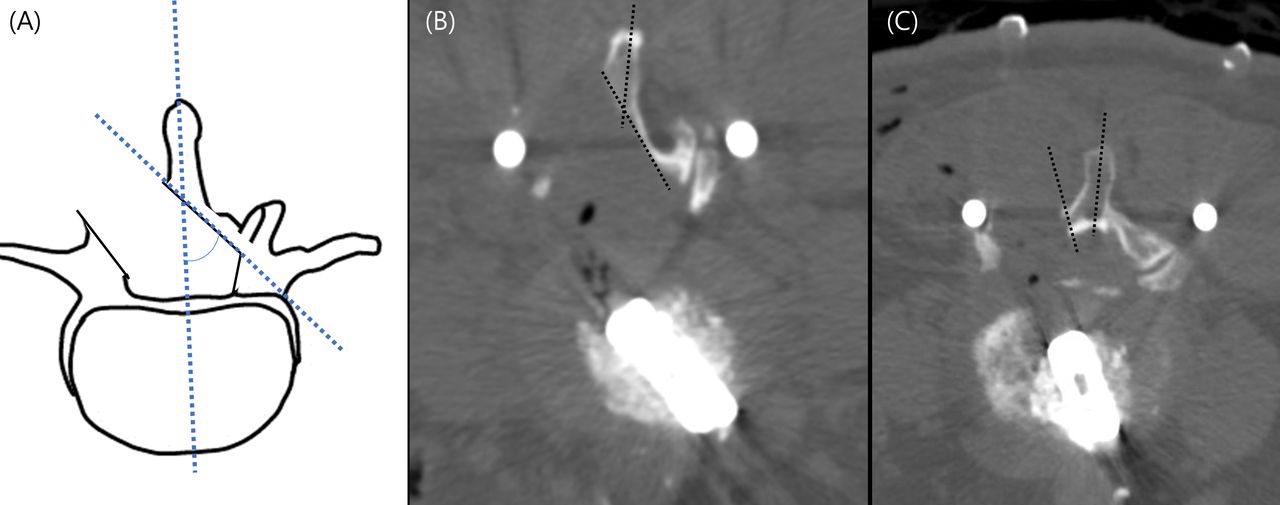
The patients’ demographics (age, sex, height, weight, body mass index, American Society of Anesthesiologists score, presence of osteoporosis, and HbA1c) and clinical factors (preoperative diagnosis, surgical level, preoperative DH, spondylolisthesis slip, presence of kissing spine, and spinopelvic parameters including pelvic incidence [PI], pelvic tilt [PT], and lumbar lordosis [LL]) were reviewed. Additionally, surgical factors such as total operation time, time spent on ULBD and cage insertion, cage size, cage angle, and final cage height were examined. Postoperative radiological factors were assessed using standing radiography at 3 months postoperatively and computed tomography (CT). These included SL correction, anterior, posterior, and mean DH elevation, slip reduction, final PI-LL, postoperative PT decrease, incidence of endplate injury, and the sublaminar decompression angle. The mean DH was calculated as the average of the anterior and posterior DHs.22 The sublaminar decompression angle is a novel concept that refers to the angle between the spinous process and the decompressed contralateral sublaminar space’s bony contour, measured on axial CT (Figure 5).

(A) The sublaminar decompression angle: the angle between the spinous process and the bony contour of the decompressed contralateral sublaminar space. (B) Axial computed tomography (CT) image of biportal endoscopic transforaminal lumbar interbody fusion (TLIF) at L4–L5 with an expandable cage. The sublaminar decompression angle is 36°. (C) Axial CT image of tubular minimally invasive TLIF at L4–L5 with an expandable cage. Only ipsilateral facetectomy was performed, and the sublaminar decompression angle is 8°.
Statistical Analysis
All data were analyzed using REX version 1.0 (Rexsoftware, Korea).
Results
All surgeries were completed without deviations from the surgical plan. The diagnoses included 7 levels of degenerative spondylolisthesis with severe spinal stenosis (Schizas grade D) and 3 levels of foraminal stenosis that had failed conservative treatment. Two of the foraminal stenosis cases were revision surgeries. Patients’ demographics and clinical factors are summarized in Table 1.
The preoperative demographic and radiographic data.
One patient underwent a 2-level BE-TLIF with expandable cages, while 4 patients had additional decompression at adjacent levels. The average total surgery time was 286 minutes, with an average of 153 minutes from ULBD to cage insertion. All cases included a contralateral partial facetectomy and a cage expansion trial.
Postoperative standing x-ray images showed a mean segmental lordotic gain of 5.4° and a mean DH increase of 3.5 mm, with an anterior DH increase of 4.8 mm and posterior height increase of 3.1 mm. Consequently, lumbar lordosis improved by 3.0°. The mean final PI-LL mismatch was 1.2°, and the PT decreased by 2.2°. Two patients did not achieve a PI-LL mismatch of less than 10 degrees, as the procedures involved primarily 1-level fusions.
Postoperative CT images revealed no iatrogenic endplate injuries. The sublaminar decompression angle averaged 31.6°, providing sufficient bilateral decompression without resecting the spinous process or requiring a contralateral approach (Table 2).
The operation related data and postoperative radiographic data.
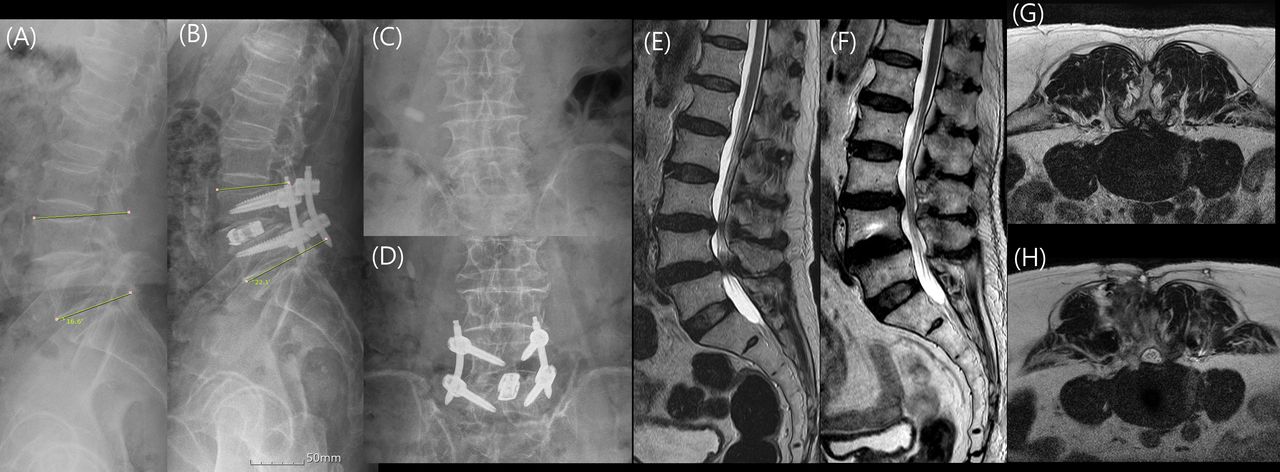
For example, the patient in case 2 underwent BE-TLIF L4 to L5 with expandable cage and BE decompression L3 to L4. The SL correction was 5.5°. The postoperative CT image of this case is shown in Figure 5. Postoperative 6-week magnetic resonance images showed a fully decompressed central canal (Figure 6).

(A and B) Preoperative and postoperative 3-month lumbar standing lateral x-ray images. (C and D) Preoperative and postoperative 3-month lumbar standing anteroposterior x-ray images. (E and F) Preoperative and postoperative 6 weeks magnetic resonance images (MRIs), sagittal cut. (G and H) Preoperative and postoperative 6 weeks MRIs, axial cut of endoscopic fusion level, L4–L5.
Discussion
This study presents the technique of BE-TLIF using a lordotic expandable cage and evaluates the outcomes in terms of SL achievement and DH elevation. Concerns have been raised that MIS-TLIF with expandable cages may achieve greater SL and DH elevation compared with static cages.23,24 However, our study, though small, demonstrated an average SL correction of 5.1° and a DH elevation of 3.5 mm.
The SL correction observed in this study is comparable to the 5.04° reported in a meta-analysis of MIS-TLIF using expandable cages.25 However, the DH elevation in our study (3.5 mm) exceeds the 1.14 mm reported in that same meta-analysis.25 When considering anterior and posterior DH separately, our results align with findings from other studies.9 These data suggest that BE-TLIF with an expandable cage can be a favorable option for achieving SL restoration and DH elevation.
Previous studies have highlighted some limitations of MIS-TLIF with expandable cages. One of the key limitations is that bilateral annulotomies and anterior longitudinal ligament resection are more critical for SL correction.26 Another issue is that cage expansion without sufficient release of the intervertebral space can lead to cage subsidence and loss of SL and DH.27,28 While our procedure shares the first limitation as a posterior approach, the outcomes differ from previous MIS-TLIF procedures for a few reasons.
Key Factors for SL Achievement and DH Elevation in BE-TLIF With Expandable Cages
Lordotic Cages
In our study, we used lordotic cages with angles of 12° and 20°. Past studies have suggested that the degree of cage lordosis was not critical to SL, but those studies involved cages with less than 12° of lordosis.29,30 Recent findings indicate that hyperlordotic expandable cages (12+ degrees) should be used to achieve SL correction and DH elevation.9,24,30 These cages, with more aggressive angles, are relatively difficult to be inserted due to its initial height in conventional MIS-TLIF. However, their use in BE-TLIF is further facilitated by the nature of the procedure, including better endplate preparation and bilateral partial facetectomies, which are discussed below.
Endplate Preparation
During BE-TLIF, endoscopic visualization allows for thorough cartilaginous endplate curettage, which reduces the risk of acute endplate injury, a key factor in preventing cage subsidence.31 Cage expansion using a torque-limited driver, combined with proper endplate preparation, ensures maintenance of SL correction and DH elevation.
Bilateral Facetectomies
Bilateral partial facetectomies in BE-TLIF, as demonstrated by the sublaminar decompression angles, facilitate the resection of the contralateral facet joint and partial removal of the SAP. This is made more effective with the use of a 30° endoscope and helps avoid resecting the spinous process. While contralateral facetectomies can be performed in MIS-TLIF using tubular retractors, they are more challenging due to limitations posed by the spinous process, often requiring additional incisions.32–34 A cadaver study has shown that adequate decompression of the posterior complex, including bilateral facetectomies, is important for achieving SL.35 Furthermore, bilateral facetectomies can aid in inserting hyperlordotic cages and avoiding endplate breakages by providing better release of the posterior disc space.27 Conversely, relying on unilateral facetectomy alone carries the risk of endplate breakage during cage expansion.28
Lumbar Lordosis and PI-LL Mismatch
Our study showed an increase in lumbar lordosis of 3.0°, and 2 patients failed to achieve a PI-LL mismatch correction of less than 10°, similar to other studies involving hyperlordotic cages.9,28,36 Most of the procedures were single-level fusions, and we performed decompression only at the levels of spinal stenosis due to insurance coverage limitations.
Surgical Approach and Incisions
We sometimes used the quarterback incisions for several reasons. The midline incisions allow for versatility, such as performing adjacent level decompressions, inserting the endoscope for cage insertion, and preventing dura injury during cage placement by allowing root retractors. After cage insertion, a temporary drain can be placed via the midline incisions to prevent hematoma formation. The quarterback incisions are small, and it does not cause muscle belly injury because it is near the spinous process.
Sublaminar Decompression Angle
The concept of the sublaminar decompression angle, typically over 30° in most cases, was introduced to assess the effectiveness of ULBD. This angle represents that the BE-TLIF facilitates bilateral synovectomies and resections of both side IAP and SAP, enabling full contralateral decompression and foraminotomy, which may help prevent complications such as contralateral radiculopathy infrequently seen in MIS-TLIF procedures.37,38 In our study, no cases of contralateral radiculopathy occurred, likely due to thorough decompression and facetectomies.
Limitations
A significant limitation of this technique is the longer surgical time, which is a critical factor in MISS. Shorter surgical times reduce the burden on elderly patients and those with comorbidities.39 Moreover, further reductions in surgical time may enable awake spine fusion surgeries performed with regional anesthesia.13,40,41 As the author gains more experience with BE-TLIF, surgical times may decrease, potentially enabling awake spine fusion techniques.
This study itself has several limitations. First, it is a technical note with preliminary results on SL achievement and DH elevation, with only a 3-month follow-up. Long-term follow-up is needed to assess potential complications, such as late cage subsidence or low fusion rates. Additionally, the small number of cases limits the generalizability of the results. Finally, the study does not prove that BE-TLIF can achieve better SL correction than tubular MIS-TLIF, nor does it suggest superiority over other fusion techniques. A comparative study between BE-TLIF and tubular MIS-TLIF is planned.
Conclusion
BE-TLIF with an expandable cage may offer benefits in SL correction and DH elevation. These advantages are attributed to the use of hyperlordotic expandable cages, combined with contralateral facetectomies and careful endplate preparation—key features of the BE-TLIF technique.
Footnotes
Funding This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT; No. 2022R1A2C1010962).
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Research Ethics As this was a retrospective case–control study reviewing patients’ medical records after surgeries, consents to participate in this study were exempted. This study was reviewed by the IRB in our hospital (30-2024-49, SMG-SNU BMC IRB).
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.