


Abstract
Introduction Recurrent lumbar disc herniation (rLDH) remains a challenge in spinal surgery. This systematic review analyzes the use of transforaminal endoscopic discectomy (TFED) for the treatment of rLDH.
Methods A comprehensive search of 4 electronic databases, including PubMed, Google Scholar, Science Direct, and Cochrane, was conducted. Studies that analyzed the use of TFED to manage rLDH were included in the review. The primary outcomes assessed in these studies encompassed postoperative complications, length of surgery, blood loss, duration of hospitalization, pain scores, and recurrence rates.
Results Six studies met the inclusion criteria, comprising 405 patients. The mean duration of surgery was 24 to 158.74 minutes with intraoperative estimated blood loss of 0 to 34.8 mL. The mean recurrence rate was 4.4% with a 0.7% progression to fusion during the follow-up period. Durotomy was seen in 2.7% of cases. There was a 0.1% incidence of temporary nerve irritation with no permanent nerve injuries reported.
Conclusions TFED for the management of rLDH is a lateral minimally invasive technique that avoids going through scar tissue, hence associated with a short duration of surgery, minimal to no measurable blood loss, and a very low complication rate. The few studies in the literature seem to suggest that TFED should be considered in patients with rLDH without segmental instability who meet the criteria for surgery.
Level of Evidence 5.
- recurrent lumbar disc herniation
- transforaminal endoscopic discectomy
- lumbar spine
- degenerative disc disease
Introduction
Recurrent lumbar disc herniation (rLDH) presents a formidable challenge in the field of neurosurgery. It is characterized by the reemergence of symptoms following initial surgical intervention for lumbar disc herniation.1 The recurrence rates vary in the published literature but are generally within the ranges of 5% to 18%.2,3 While various surgical techniques have been employed to address this condition, the optimal approach remains a topic of debate. Traditional options include repeat microdiscectomy and fusion procedures, such as transforaminal lumbar interbody fusion (TLIF).2,4–7 The risk of injury to the dura and nerve root due to adhesions and scar tissue, recurrence, and the progression to instability limits the use of repeat microdiscectomy, whereas TLIF, though eliminating the risk of the same recurrence, is limited by the risk of the adjacent segment disease and instrumentation associated complications.7–9 However, in recent years, transforaminal endoscopic discectomy (TFED) has emerged as a promising alternative. TFED is a minimally invasive surgical technique that offers precise visualization and targeted removal of herniated disc material while avoiding extensive tissue disruption.10,11 Although TFED has demonstrated efficacy in treating primary lumbar disc herniation, its role in managing rLDH has not been comprehensively explored.12
This systematic review aims to evaluate the existing literature on TFED as a surgical option for rLDH, shedding light on its efficacy, safety profile, and potential advantages in comparison to traditional approaches. By synthesizing the available evidence, we seek to provide valuable insights into the role of TFED in contemporary neurosurgical practice and contribute to the ongoing discussion regarding the optimal management of rLDH.
Methods
Information Sources and Search Strategy
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, we conducted a search of terms in the PubMed/Medline, Cochrane, and Embase databases. We used the patient/population, intervention, comparison and outcomes format:
Population: Patients receiving treatment for rLDH at the same level.
Intervention: TFED.
Comparison: None.
Outcome: Any.
Subsequently, search terms were further refined using Medical Subject Headings to expand the keywords. Data search was conducted up to and including 2023.
Inclusion and Exclusion Criteria
To be eligible for inclusion, articles had to meet the following criteria: (1) the study population included patients with rLDH; (2) the study discussed TFED for the treatment of rLDH; (3) sample size of at least 10 patients; and (4) published in or translated into English. Articles were excluded if they met any of the following criteria: (1) the study population included only pediatric cases; (2) case reports or technical reports; and (3) not published in English or lacked an English translation.
Study Selection, Data Extraction, and Quality Assessment
Two authors (G.M. and N.A.) independently screened the titles and abstracts of selected articles to determine their eligibility. The full text of potentially relevant articles was then reviewed to confirm compliance with the requirements. Two authors (G.M. and N.A.) independently assessed the quality of the included studies. This was performed for each study using the Newcastle–Ottawa Scale adapted for cross-sectional studies. Extracted data included (1) demographic characteristics of the study population; (2) clinical characteristics of the study population; (3) surgical details, including complications, and duration of surgery; (4) length of hospitalization; (5) pain scores; and (6) recurrence rates. After the data extraction form was developed, 2 authors (G.M. and N.A.) dependently extracted the data from included studies. Any discrepancies in data extraction were solved by a third author (N.M.).
Results
Study Selection
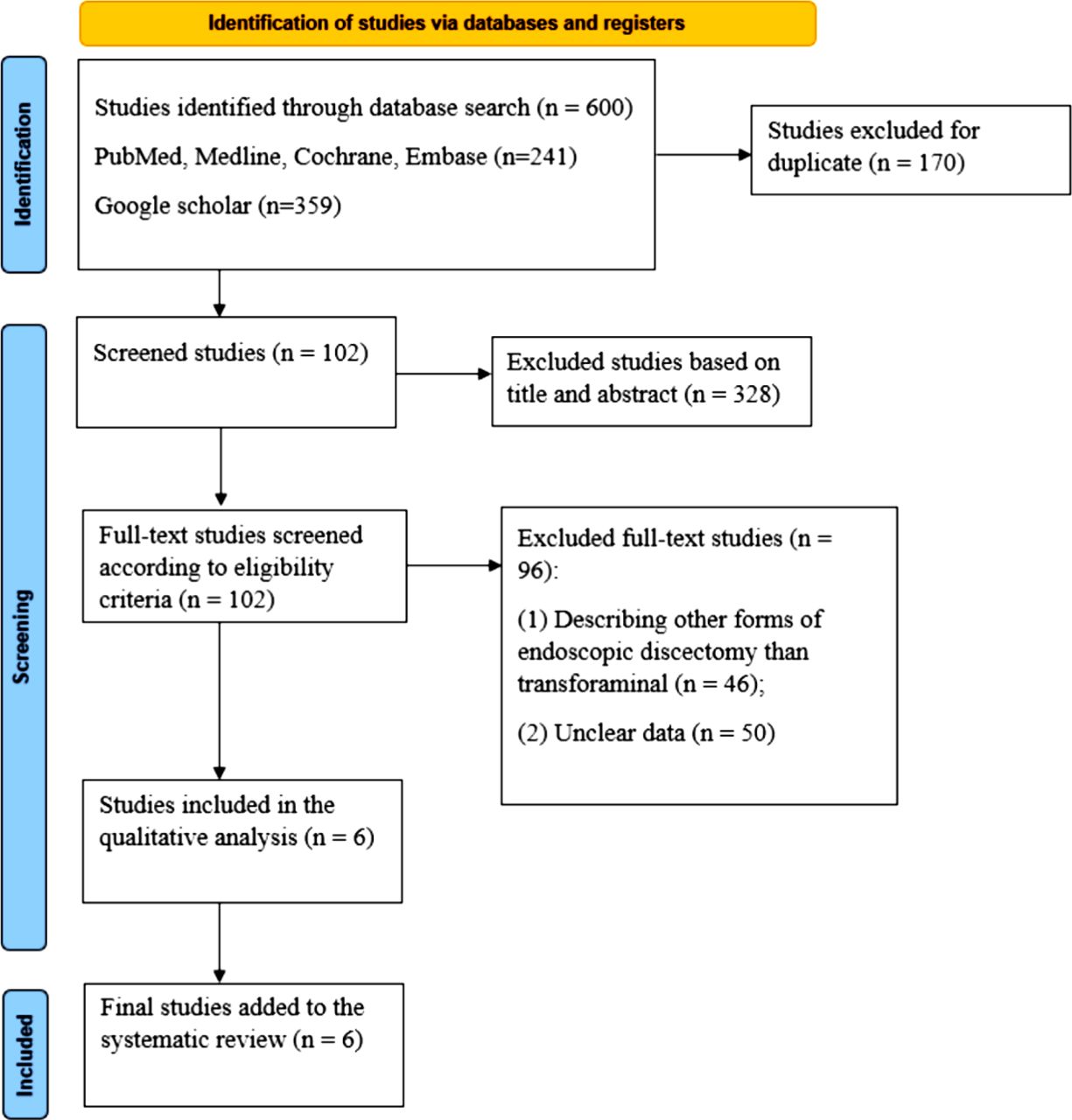
Initially, a database search yielded 600 articles related to the topic. Subsequently, 170 duplicates were removed, leaving 430 articles. Titles and abstracts were then analyzed, resulting in the selection of 102 articles. Finally, after a full-text review, 96 articles were excluded due to unclear data, describing other forms of endoscopy other than transforaminal, or unavailability of the full text. The last 6 articles met our inclusion and exclusion criteria. A total of 405 patients underwent TFED for rLDH (Figure). Six studies (2 prospective and 4 retrospective) with 405 patients were analyzed. Of note, the included studies did not report all the variables studied in the present review. There was significant inconsistency in the reporting of data in the literature, making analysis a challenge.

Study selection according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Intraoperative Parameters
Only 3 of the 6 studies (50%) reported the duration of surgery (defined as the time from incision to placement of the last suture), which ranged from 24 to 158.74 minutes. When duration of surgery is reported in the literature, it presents great variability because the factor of surgeon experience is rarely considered. Logically, more experienced centers are likely to have a shorter duration of duration than institutions with lower experience or training centers with residents. Blood loss data were available in 3 studies (50%). There is significant variability in the reported intraoperative blood loss ranging from 0 to 34.8 mL. One study reported unmeasurable intraoperative blood loss, although it is highly unlikely to have 0 mL blood loss in the presence of an incision regardless of size. TFED is a minimally invasive surgery with a 1 cm incision; hence, minimal blood loss is expected. Four out of the 6 articles (66.7%) reviewed reported on durotomy. There were no cases of incidental durotomies reported in the review. TFED allows for direct visualization of the dura and nerve root without traversing the adhesions significantly reducing the risk of durotomies (Table 1).
Analysis of intraoperative parameters.
Intraoperative and Postoperative Complications and Hospital Stay
Postoperative hospital stay was reported in only 2 studies, ranging from 1 to 5.9 days. No permanent nerve injuries were reported, but the rate of temporary nerve irritation was 0.1% (4 cases). The commonly affected nerve root was the traversing previously compressed nerve, not the healthy exiting nerve. In these patients, nerve root irritation regressed with conservative treatment. Only 1 patient required a nerve block to achieve complete regression of symptoms. The presence of postoperative irritation was attributed to postoperative edema of the nerve root due to manipulation or reperfusion.
Out of 6 studies, 5 (83.3%) reported on the development of recurrence, with an overall recurrence rate of 4.4%. One study reported a high recurrence rate of 20.8%. It should be noted that the definition of recurrence varied across the articles reviewed. For instance, Hoogland et al considered all recurrences within the first 3 months as postoperative complications and not true recurrences.10 In their study, 6 patients had early (within 3 months) rLDH (6/262, 3.44%), 1 patient after 1 day (because he slipped in the shower), 1 patient after 6 days, 1 patient after 12 days, 2 patients after 4 weeks, and 1 patient after 12 weeks. They reported another 11 (4.62%) patients as true recurrences after 3 months. Of these patients, only 1 underwent fusion during the follow-up period, while the others were managed with repeat endoscopic discectomy or microdiscectomy.10 Wang et al13 and Ruetten et al11 did not specify a criterion for recurrence. Among patients with recurrence, progression to fusion surgery during the follow-up period was 0.7% (Table 2). The management of recurrence varies from institution to institution. Wang et al13 managed 3 patients conservatively with good response, and 2 patients needed fusion surgery. There were no clear indications to choose 1 repeat surgical technique over the other.
Analysis of intraoperative and postoperative complications.
Postoperative Pain and Quality of Life
Pre- and postoperative visual analog scale (VAS) pain scores were reported in all the analyzed studies. The highest preoperative VAS score reported was 8.72 ± 1.20, compared with the lowest postoperative score of 0.43 ± 0.26. The VAS scores were recorded at various intervals in the 6 studies reviewed. Preoperative and last postoperative follow-up VAS scores were analyzed. The mean preoperative VAS was 7.77 ± 108 cm compared with 2.11 ± 1.08 cm postoperatively with an average change of 5.66 ± 2.16 cm. Oswestry Disability Index (ODI) scores were reported in 3 of the 6 studies (50%) to assess the effect of surgery on the quality of activities. The highest recorded preoperative ODI was 39.87 ± 7.65, compared with the postoperative ODI of 2.61 ± 1.55 (Table 3). The mean preoperative ODI was 36.34 ± 5.88 compared with 8.09 ± 3.88 postoperatively with an average change of 28.25 ± 2.
Postoperative pain and quality of life.
Discussion
rLDH poses a persistent and intricate challenge in clinical settings, and the most effective surgical approach for managing this condition continues to be a subject of active discussion. In addressing this clinical conundrum, our systematic review sought to comprehensively assess the efficacy and safety of TFED as a viable treatment option for rLDH. By delving into the outcomes and implications of TFED, we aim to contribute valuable insights into its role within the framework of contemporary neurosurgical practices, shedding light on its potential benefits and considerations for clinicians and researchers alike. Revision surgery is needed for most patients who suffer from recurrent low back pain or lower limb symptoms after percutaneous endoscopic lumbar discectomy if conservative treatment fails to relieve the patient’s symptoms. However, few studies have evaluated the clinical outcomes of reoperation surgery after percutaneous endoscopic lumbar discectomy, relative to primary open surgery, for treating symptomatic lumbar disc disease. Outcomes of revision lumber open surgery tend to be worse than the initial procedure when there is a dural tear, nerve root injury, and other complications, which may be due to epidural or nerve root scarring from the first surgery.16–18
Efficacy of TFED and Safety Profile
This systematic review underscores TFED as a viable and promising surgical option for rLDH. Our comprehensive analysis of the existing literature suggests that TFED can yield favorable outcomes, achieving symptom relief and functional improvement that stands on par with conventional surgical methods such as microdiscectomy, with or without fusion. The distinctive advantage of TFED lies in its minimally invasive approach, allowing for precise visualization of the herniated disc and targeted removal of pathological tissue, thereby facilitating effective decompression of neural structures.19–21 Examining multiple studies included in this review reveals consistently positive clinical outcomes post-TFED. Notably, these outcomes include a significant reduction in early postoperative pain, with VAS scores as low as 0.43 ± 0.26 cm. Long-term assessments further demonstrate substantial improvements in patients’ quality of life, with a decrease of 17 to 43 points in ODI scores13,14 when compared with preoperative scores.
A notable advantage of TFED lies in its highly favorable safety profile. Noteworthy aspects of this safety profile include minimal and even unmeasurable11 intraoperative blood loss, abbreviated hospital stays, and a reduced incidence of complications. Importantly, TFED distinguishes itself by eliminating the need for hardware implantation, mitigating concerns related to adjacent segment degeneration and pseudoarthrosis—issues commonly associated with fusion surgery.3,6,7,22–24 The minimally invasive approach of TFED also manifests in less disruption to paraspinal musculature, a factor that holds promise for minimizing the risk of postoperative back pain and instability. Furthermore, the low risk of temporary nerve irritations due to reperfusion edema after decompression,10,13 coupled with the absence of permanent neurological deficits, underscores the safety profile associated with TFED.
Patient Selection and Considerations
The efficacy of TFED in addressing rLDH is contingent upon careful patient selection and consideration of specific factors. Notably, patient characteristics such as the presence of Modic changes and the degree of segmental instability emerged as pivotal considerations influencing the choice of surgical technique.12 Establishing clear indications for the use of TFED in rLDH cases is imperative, serving to optimize outcomes and curtail the risk of recurrence.
The risk of repeat recurrence remains a significant complication in these patients as every subsequent surgical intervention on the spine is associated with worse outcomes, especially with regard to worsening postoperative pain.25 There is no standard definition of recurrence in the literature. Hoogland et al10 did not consider recurrences within the first 3 months as true recurrences but reported it as postoperative complications. Other authors consider 1 month as cut-off.4 There is a need to clearly define this period to standardize reporting in the literature. Our analysis revealed a relatively low recurrence rate of 4.4%, with 0.7 % progression to fusion surgery. There is no clear indication as to when it is necessary to perform fusion after a failed discectomy. In this review, repeat TFED or microdiscectomy was the most performed revision surgery. Three patients were managed conservatively using steroids and nonsteroidal anti-inflammatory drugs with good response.15 However, the indications for this decision were not clearly outlined. This stands in stark contrast to higher recurrence rates reported for alternative techniques, such as repeat microdiscectomy.8,9,26–28 These findings accentuate the importance of strategic patient selection and the nuanced application of TFED in managing rLDH, suggesting its potential as a preferred and effective surgical modality in appropriately chosen cases.
Comparison With Other Minimally Invasive Techniques
While TFED offers distinct advantages, it is crucial to compare its efficacy and safety with other minimally invasive techniques such as microendoscopic discectomy (MED) and minimally invasive TLIF (MI-TLIF). Studies indicate that MED and MI-TLIF also yield favorable outcomes for rLDH, but with different risk profiles. For instance, MED is associated with shorter recovery times and reduced blood loss similar to TFED, but MI-TLIF may be preferred in cases with significant instability, providing the benefit of fusion while still being minimally invasive.29,30
Postoperative Rehabilitation
An often-overlooked aspect of postoperative care is the role of rehabilitation in enhancing recovery and minimizing recurrence. Early mobilization, combined with a structured physical therapy program, can significantly improve functional outcomes and reduce the incidence of postoperative complications. Rehabilitation protocols should be individualized, focusing on core strengthening, flexibility exercises, and ergonomic training to prevent further disc degeneration and promote spinal health.31,32
Cost-Effectiveness, Long-Term Outcomes, and Recurrence Prevention
The incidence of recurrent disc herniation has been reported to be around 5% to 18% in patients after open lumbar surgery.25,30 Recurrent disc herniation is thought to be the major cause of surgical failure after open lumbar surgery, especially after microdiscectomy procedure. The cost-effectiveness of TFED compared with traditional open surgeries and other minimally invasive techniques is a crucial consideration, particularly in healthcare systems with constrained resources. TFED typically results in shorter hospital stays, reduced need for postoperative analgesics, and quicker return to work, all contributing to its overall cost-effectiveness. Future research should focus on long-term cost-benefit analyses, incorporating both direct and indirect healthcare costs.33–35 Long-term outcomes of TFED, including recurrence rates and the development of adjacent segment disease, remain areas of active research. Strategies to prevent recurrence include meticulous surgical techniques to ensure complete removal of the herniated disc material and addressing any biomechanical factors contributing to disc degeneration. Regular follow-up with imaging and clinical evaluation is essential to monitor for signs of recurrence or new pathology.36
Controversies, Future Directions, and Integration of 3D Printing in TFED
While the studies encompassed in this review present promising outcomes for TFED in managing rLDH, the literature remains embroiled in ongoing controversies regarding the optimal surgical approach for this condition. Divergent viewpoints persist, with some neurosurgeons favoring repeat microdiscectomy for its minimally invasive nature and cost-effectiveness, while others advocate for fusion techniques, particularly in cases with apprehensions about recurrent instability.4,21,28–37
Future research endeavors should prioritize the refinement of patient selection criteria for TFED, aiming to identify predictive factors for treatment success. Comprehensive long-term follow-up studies are imperative to ascertain the durability of symptom relief and evaluate the risk of re-recurrence associated with TFED. Furthermore, there is a critical need for comparative studies directly pitting TFED against other surgical approaches for rLDH.38
An emerging topic is the integration of 3-dimensional (3D) printing technology in TFED. 3D printing can revolutionize preoperative planning and intraoperative guidance in spinal surgery. Customizable 3D-printed models of the patient’s spine, created from preoperative images, can provide surgeons with a detailed anatomical replica, aiding in precise surgical planning and simulation.39–41 These models can help identify optimal entry points, navigate complex anatomies, and avoid critical structures, enhancing the accuracy and safety of TFED procedures. Moreover, 3D-printed guides and templates can be utilized intraoperatively to ensure accurate instrument placement and trajectory, further minimizing risks and improving outcomes. Personalized 3D-printed implants tailored to the patient’s anatomy could also be developed, offering enhanced fit and integration compared with standard implants. While 3D printing in spinal surgery is still in its early stages, its potential to enhance TFED and other minimally invasive techniques is significant, warranting further exploration and research.42,43
Limitations
While this systematic review provides valuable insights into the use of TFED for rLDH, several limitations should be acknowledged. First, only 6 studies met the inclusion criteria, which limits the generalizability of the findings. A larger number of studies would provide a more robust evidence base. Second, the included studies varied significantly in terms of study design, patient populations, and outcome measures. This heterogeneity makes it challenging to perform a meta-analysis and draw definitive conclusions. Third, not all studies reported on all the outcomes of interest, such as duration of surgery, blood loss, or postoperative complications. This incomplete reporting can introduce bias and affect the overall analysis. In addition, the follow-up periods varied among the studies, with some studies not providing long-term follow-up data. Longer follow-up is necessary to accurately assess the recurrence rates and long-term outcomes of TFED.
There was no standardized definition of recurrence among the studies. Different criteria for what constitutes a recurrence could affect the reported recurrence rates and complicate comparisons between studies. Finally, some studies were conducted at single centers, limiting the generalizability of the findings to broader, more diverse patient populations.
Conclusions
TFED for the management of rLDH is a lateral minimally invasive technique that avoids going through scar tissue, hence associated with a short duration of surgery, minimal to no measurable blood loss, and a very low complication rate. The few studies in the literature seem to suggest that TFED should be considered in patients with rLDH without segmental instability who meet the criteria for surgery.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2025 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.