


Abstract
Background Transforaminal lumbar interbody fusion (TLIF) achieves anterior and posterior spinal arthrodesis through a single approach. Minimally invasive surgery (MIS) methods reduce surgical morbidity while achieving positive outcomes.
Methods The major MIS-TLIF techniques, from tubular to endoscopic approaches, are reviewed with a discussion on the incorporation of new technologies and a comparative review of their outcomes.
Results MIS-TLIF approaches span a spectrum of visualization methods, with technical nuances related to patient and surgeon-specific factors determining optimal fit. To date, the superiority of 1 technique has yet to be definitively determined. Existing techniques may be integrated in a personalized manner to optimize surgical utility.
Conclusions Selection of an MIS-TLIF modality relies on a calculus between patient characteristics and surgeon faculty; proper selection can offer significant benefits to patients with spine disease.
Clinical Relevance Emerging technologies for MIS-TLIF comprise a major source of development and clinical translation, while the safe and effective use of these techniques promises greater patient benefit in the right populations.
Introduction
A major goal of spinal fusion surgery is to achieve durable arthrodesis within the framework and rigid fixation provided by instrumentation. To that end, accessing the anterior column with interbody fusion techniques capitalizes on a large surface area and load-sharing properties to achieve successful fusion. The transforaminal lumbar interbody fusion (TLIF), as first described by Harms and Rolinger, accesses this space through a safe corridor defined as Kambin’s triangle.1,2 A thorough understanding of the safe working window within this space is crucial for effectively performing TLIF; the original description, therefore, has been further delineated as Kambin’s prism to better characterize the 3-dimensional topography of the complex.3 As part of the increasing rate of interbody fusions being performed in the United States, TLIFs represent a crucial option for achieving fusion.4
Broadly, TLIF procedures provide direct decompression of the neural elements, similar to that of a posterior lumbar interbody fusion, but avoid the potential complications associated with bilateral nerve root retraction and disc space exposure. Moreover, when compared with anterior lumbar interbody fusion and lateral lumbar interbody fusion approaches, they avoid the potential complications involving abdominal viscera, major vasculature, as well as lumbosacral and sympathetic plexuses. However, traditional open dissection techniques for lumbar fusions lead to significant injury, with lasting impacts on surrounding soft tissue and musculature. A major cause of postoperative morbidity from open surgery is the impact of electrocautery dissection and self-retaining retractor placement on atrophy and scarring within the paraspinal musculature, which often results in higher blood loss, postoperative pain, and de-conditioning.5–7
To reduce this unintended surgical footprint on the patient’s normal anatomy, minimally invasive surgery (MIS) TLIF techniques have been developed. Dissection utilizing a paraspinal Wiltse approach provides an atraumatic, natural corridor to the facet and transverse process.8,9 Following the sentinel advent of the tubular retractor and serial dilation approach for MIS-TLIF by Foley et al, the MIS-TLIF has evolved to feature a multitude of retractor and visualization systems that reduce retraction-associated tissue injury and improve navigation within Kambin’s triangle.10–13 The growing use of enabling technologies, such as endoscopy, image-guidance, and robotics, continues to further push the boundaries of the MIS-TLIF procedure. In this review, we provide a detailed technical description of 2 major TLIF approaches—the tubular and endoscopic TLIF—followed by a discussion on augmentative technologies, anesthetic considerations, and modality-comparative TLIF outcomes.
The Tubular TLIF Technique
Standard to any TLIF surgery, tubular MIS-TLIF is performed prone with general anesthesia and neuromonitoring with motor/sensory-evoked potentials and electromyography. Although there may be variations in surgeon preference for adjusting positioning during the decompression and instrumentation portions of surgery, the ultimate procedural goal will be to position the patient in a manner that helps optimize lordosis or achievement of correction. The senior author’s preference is for a standard Jackson table to that end to maintain lordosis. Anteroposterior (AP) and lateral fluoroscopy are used to localize the correct level of pathology. It is crucial to obtain high-quality sets of images in both planes: anteroposterior imaging show midline spinous processes, parallel endplates, and equidistant pedicles, while lateral imaging demonstrates superimposed pedicles and the absence of any double-shadow effect on endplates; moreover, the area of interest must be kept in the center of the image to avoid parallax effect. Positioning must therefore be optimized prior to beginning the case for optimized technician-surgeon workflow and surgical efficiency.
The entry point of the trajectory to the facet is then marked on the skin, which often measures between 4 and 5 cm lateral to midline, although this can vary depending on the trajectory chosen and the patient’s body habitus. A large habitus may warrant a more lateral starting point, whereas a smaller patient may necessitate a medial starting point. Of note, a more medial starting point may be beneficial as part of an interlaminar approach targeting the laminar-facet junction vs a more lateral starting point directed toward a trans-facet approach that targets more laterally on the facet complex itself. Significant facet arthropathy and regional pathology are taken into consideration during preoperative planning to ensure that appropriate localization is performed for the starting point.
Once the entry point is identified, a 2- to 3-cm skin incision is carried, and dissection with electrocautery is carried down to the fascia, which is incised along the entire length of the incision to avoid tube entrapment or restrictions in movement to ensure early hemostasis. The intermuscular plane, where an initial dilator will be introduced, is identified. Blunt dissection through this natural Wiltse plane between the multifidus and longissimus muscles is first performed with a finger to the facet-transverse process junction. This process helps to minimize muscular trauma and bleeding while allowing for the initial dilator to be easily docked onto the facet. Serial dilation is then performed over the initial dilator. A counterclockwise followed by clockwise twisting motion will help reduce the amount of muscle creep into the operative corridor. The optimal tube length should be to the level of the skin incision. The tubular retractor is then placed over the final dilator system and secured to a table-mounted retractor arm whose positioning is kept away from the surgical field and off the patient. Correct positioning of the docked working channel should be confirmed on AP and lateral fluoroscopy. The optimal diameter of the tube will be the smallest size that the surgeon can safely and efficiently perform the procedure without excessive tissue manipulation. The size commonly ranges from 21 to 26 mm. In variations of this approach, an expandable tubular retractor (eg, “mini-open”) or camera-integrated tubular retractor system can aid in allowing for equal ease of performing the procedure using smaller diameter tubes, which are often 15 mm in size.14,15 Here, the senior author determines the visualization modality based on patient-specific factors such as habitus, the ability to tolerate prone surgery, and whether angled visualization (eg, camera) or linear visualization (eg, microscope or loupes) is necessary.
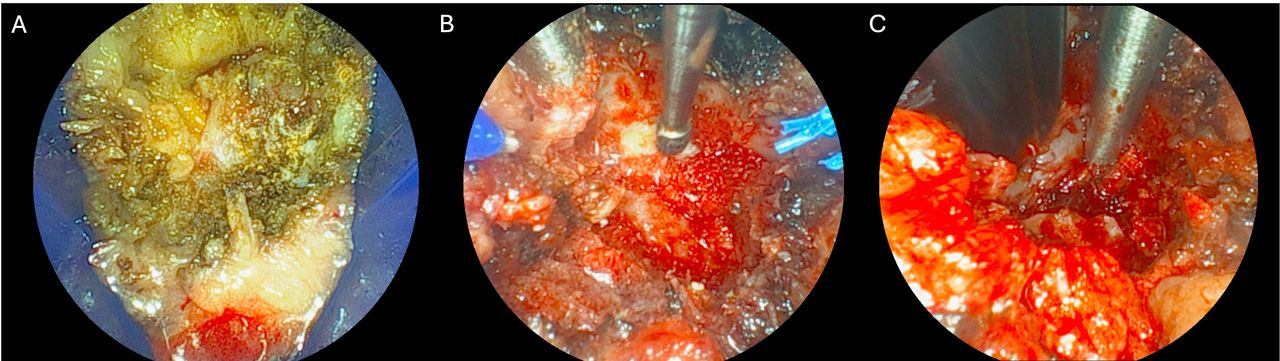
In the authors’ direct tubular experience, dilators are then removed, and either a microscope or loupes will be used to magnify visualization inside the tubular retractor. A small amount of muscle creep is inevitable and can be removed with monopolar or bipolar electrocautery. If fine adjustments are needed for tube positioning, the largest dilator can be re-placed inside the tube before adjusting to avoid accidental tissue encroachment into the operative corridor. Fluoroscopy is repeated to ensure appropriate positioning to provide a road map prior to further tissue manipulation. At this point, one must be fully oriented to the visualized anatomy. Ideally, the location of the inferior edge of the rostral lamina, pars, and facet joint should be identified. At the very least, clear visualization of the facet joint should be apparent (Figure 1).

Example of tubular minimally invasive surgery transforaminal lumbar interbody fusion performed on right side. Case demonstrates a tubular system with integrated 22.5° camera for visualization. Image orientation: top, medial; bottom, lateral; left, caudal; and right, cranial. (A) Facet joint complex visualization after initial soft tissue dissection. (B) Facetectomy, hemilaminotomy, and exposure of ligamentum flavum. (C) Lateral edge of thecal sac and traversing nerve root visualized after resection of ligament.
Several approaches to bony removal may be taken. One method is to use a combination of high-speed drill, Kerrison rongeurs, or straight osteotomes to create an L-shaped medial vertical cut from the inferior lamina, followed by a transverse lateral cut through the pars. This technique allows for the removal of the inferior articulating process as a fragment of osseous autograft that can be used for arthrodesis. Another approach is to directly drill the facet by following the facet joint to the level of the disc space. In both ways, the inferior articulating process, along with the superior and medial portion of the superior articulating process, should be removed to provide a wide enough transforaminal corridor to the disc space for implant placement. The senior author’s preference on how initial decompression is done takes into consideration bony anatomy, tube placement, as well as the degree of medial–lateral decompression that will be desired. The extent of additional bony and ligamentous removal will depend on pathology such as the presence of a synovial cyst or ligamentous hypertrophy. It is possible to decompress further centrally, even to the contralateral side, and completely expose the exiting nerve roots to provide comprehensive direct decompression in addition to the indirect decompression provided by interbody placement. However, some of these steps may not be necessary unless indicated by the specific goals of surgery.
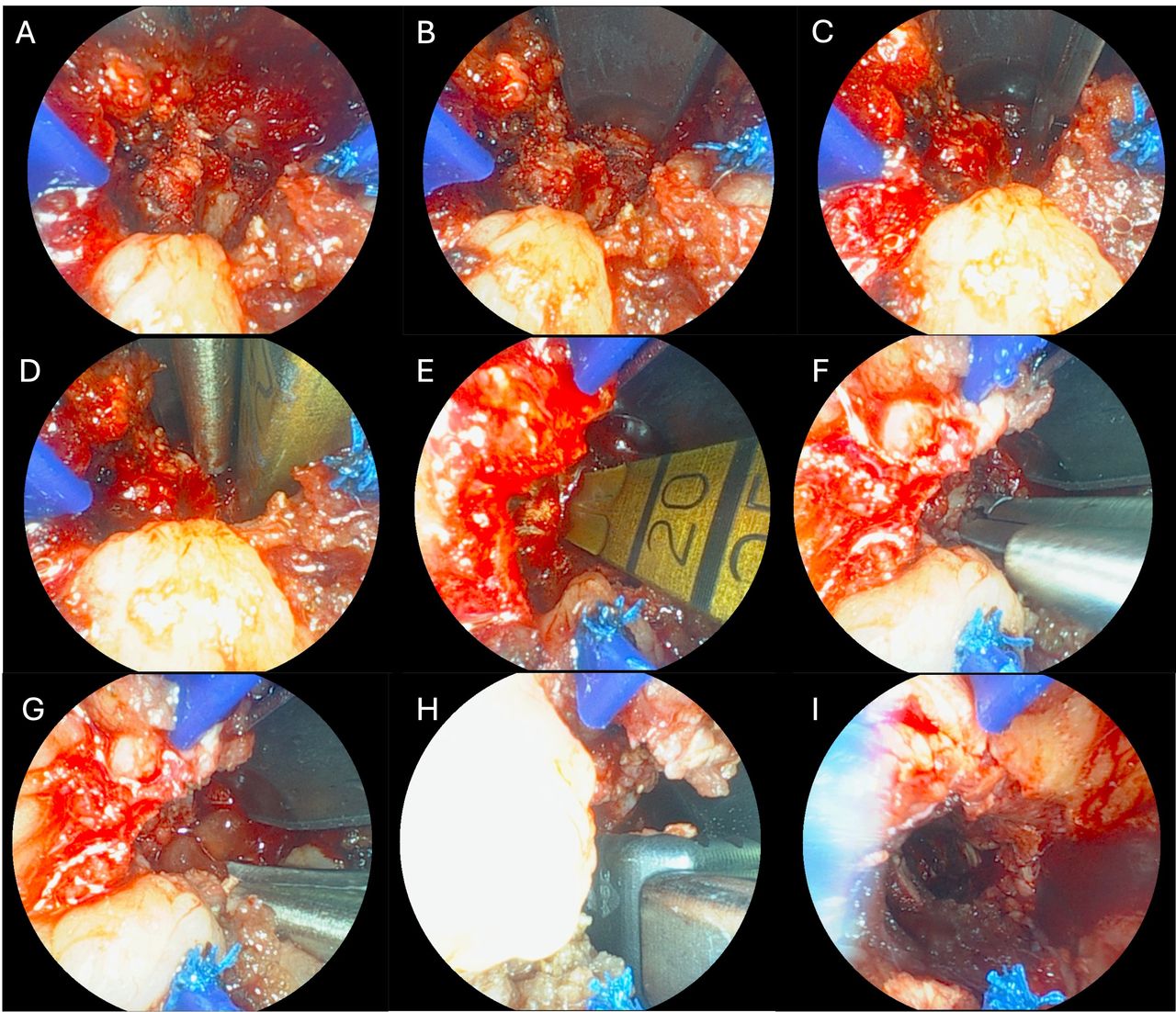
Once visualized after resection of the yellow ligament, the epidural veins over the disc space can be coagulated with bipolar cautery to minimize bleeding. An annulotomy is made with a 15 blade. As sequentially demonstrated in Figure 2, discectomy and endplate preparation are then completed with a combination of dilators, shavers, and curettes. Appropriate disc-space preparation is critical in creating an adequate environment for fusion across the interbody graft. Care and time should be spent to perform a thorough and complete discectomy, with care taken to avoid violating the cortical endplate surface to avoid the risk of cage subsidence. Vendor-specific trials may be used to help dilate the disc space and appropriately size the interbody implant. The disc space is copiously irrigated to clear any loose disc fragments after the discectomy. Autologous bone graft should then be packed in the prepared disc space, with consideration of additional osteoinductive or osteoconductive agents per surgeon preference. The specific interbody implant used is then placed in the appropriate position. Care is taken to avoid handed bias in placing the graft appropriately into the prepared disc space. Generally, an implant is preferably placed crossing midline and as anteriorly as possible to optimize cortical endplate contact and lordosis. However, specific cage placement depends again on the goals of surgery and can be modified as such. Care must be taken during discectomy and implant placement to also not unintentionally violate the anterior longitudinal ligament and enter the abdominal cavity or injure major vessels. The implant should not be oversized to reduce the risk of subsidence or endplate fracture, nor undersized to reduce the risk of cage migration.

Example of tubular minimally invasive surgery transforaminal lumbar interbody fusion performed on the right side. Disc-space preparation and interbody placement. Image orientation: top, medial; bottom, lateral; left, caudal; and right, cranial. (A) Prediscectomy visualization of transforaminal corridor. (B) Protection of the traversing nerve root with a self-retaining protector. (C) Annulotomy. (D) Initial dilator placement. (E) Tube rotation 90° clockwise and shaver introduction. (F) Disc space preparation. (G) Placement of bone morphogenetic protein. (H) Implant placement. (I) Retractor removal and final view.
Pedicle screws can then be placed in percutaneous fashion. We place pedicle screws under AP fluoroscopy. An ideal pedicle screw entry point, just lateral to the mid-lateral border of the pedicle, is visualized, and a point lateral to this is marked on the skin. Again, in obese patients, this may require a more lateral skin entry as opposed to a thin patient, in whom a more medial incision may be used. An approximately 1-cm stab incision is made. Monopolar cautery can then be used to dissect the underlying tissue and incise the fascia. This should be performed subcutaneously in a manner mimicking the pedicle screw trajectory. Next, standard percutaneous techniques are applied to place the screws. Our preference is for a single-step pedicle screw system with an integrated sharp K-wire and cutting screw tip for greater surgical efficiency and minimizing tissue trauma. The K-wire is projected approximately 5 mm, and this is docked onto the mid-lateral border of the pedicle with an AP view. A mallet anchors this in the cortical bone, and the K-wire is sequentially advanced up to 20 mm under AP guidance, taking care to not violate the medial border of the pedicle. A lateral image can be used to confirm screw passage through the pedicle into the posterior vertebral body and rostral-caudal trajectory. The remaining screw placement is completed while retracting the K-wire, and the driver is released leaving the pedicle screw in its final position. This is repeated for all remaining screw levels. An appropriately sized rod is then placed in the subfascial plane percutaneously. One should ensure that the rod is indeed subfascial to avoid muscle necrosis and pain. Set screws secure the rod, and the percutaneous towers are released from the screw heads. Reduction maneuvers utilizing the rod and towers can be applied in cases of significant spondylolisthesis.
The Endoscopic TLIF Technique
Endoscopic TLIF may utilize either uniportal or biportal approaches, which offer their own sets of advantages and disadvantages.16 Here, the authors focus on a uniportal endoscopic TLIF technique. Although this procedure is done in the prone position, for endoscopic fusion, the patient is positioned on a Wilson frame to help open the foraminal window through which the procedure is performed. Again, obtaining optimal AP and lateral fluoroscopic images of the target level as described above is important. The midline along the spinous processes along with a horizontal line parallel to the target disc space is marked. The ideal entry point is generally about 10 to 12 cm from the midline but varies depending on the patient’s body habitus. The ideal trajectory toward the disc space balances an accessible line to perform a thorough contralateral discectomy with the prevention of injury to the dorsal root ganglion (DRG). A more lateral entry point with a flatter trajectory will facilitate the discectomy, while a more medial entry point and steeper trajectory will allow for greater protection of the DRG. The senior author advocates for a more medial and steeper trajectory to avoid the postoperative dysesthesia associated with DRG injury—a notable risk of endoscopic procedures and contributor to significant postoperative pain.17 A spinal needle is then introduced from the entry point under AP fluoroscopic guidance toward Kambin’s triangle. The needle should target the safe zone between the lateral pedicle wall and the midpedicular point on AP view and just above the posterior superior endplate of the caudal vertebrae on lateral view to avoid the exiting nerve root. An overgrown superior articulating process may impede access to this space. In these circumstances, a reamer or drill may be used to create a foraminal opening to the disc space, though often the needle can be slightly re-adjusted to a steeper angle to “step around” bony anatomy.
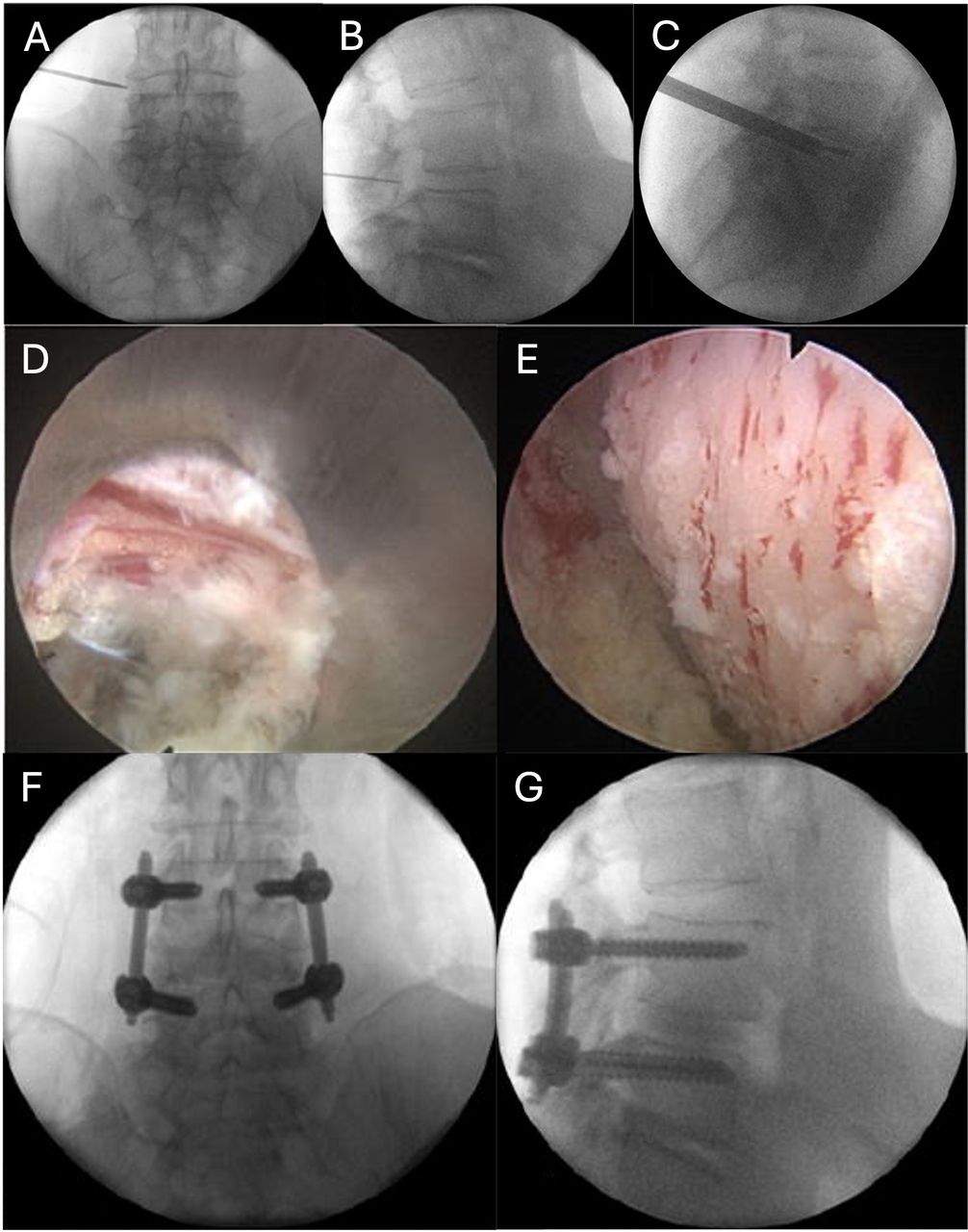
Once the entry position is confirmed at the midpedicular line, the needle can be advanced slightly further into the disc space (Figure 3). At this point, a nitinol wire is introduced into the disc space to a point spanning at least into the anterior one-third of the disc space. The needle can then be withdrawn, and serial dilation down the nitinol wire is performed. The 8-mm working cannula is then placed over the final dilator and positioned at approximately the depth of the posterior one-third of the disc space along the midpedicular line. This allows for enough access to perform the superficial portion of the discectomy while also adequately protecting the exiting nerve root and DRG. The positioning of the cannula is confirmed on fluoroscopy.

Example of endoscopic minimally invasive surgery transforaminal lumbar interbody fusion. (A) Anteroposterior and (B) lateral fluoroscopy for localization. (C) Disc space preparation through the final working channel. (D) Endoscopic view of disc space (left, bottom), traversing nerve root (right, top). (E) Endplate preparation. (F) Anteroposterior and (G) lateral fluoroscopic views of the final construct. Figure adapted with permission.15,18
The endoscope is then placed through the working cannula, and discectomy is performed under direct visualization. Pituitary rongeurs are used to remove as much disc material as possible. Interval fluoroscopy is important to know how deep the tools are being placed. After the initial discectomy, we reintroduce the nitinol wire into the disc space and replace the working cannula with the working channel associated with our interbody of choice. A side-cutting hand drill is then rotated into the disc space up to the anterior annulus under fluoroscopy. Loose fragments are subsequently removed with a pituitary rongeur. Articulating curettes can then be used to remove additional disc material and the cartilaginous endplate. A powered wire brush helps facilitate the removal of additional disc material in an efficient manner. The endoscopic working cannula is then placed again, and the adequacy of the discectomy can be assessed under direct visualization. From our experience, direct visualization of disc preparation and endplate work provides the advantage of ensuring that the cartilaginous endplate has been removed and confirming the vascular blush of the prepared cortical endplates—a crucial step in ensuring appropriate fusion occurs.
Interbody placement in endoscopic fusion is often facilitated by fluoroscopic confirmation. A contrast-injectable balloon provides another method for the surgeon to assess the completeness of the discectomy by expanding and visualizing the character of contrast filling. If additional discectomy is required, the previous discectomy steps may be repeated as needed. Osteobiologics and graft material may be then placed in the prepared disc space. The implant is then introduced into the disc space, and several prefilled bone graft channels are then impacted into the mesh-based interbody for controlled expansion of the disc space. This is carefully filled under fluoroscopic guidance. The amount of graft material can be measured by preoperative planning, visualization on fluoroscopy, and based upon the tactile feedback of graft impaction. Care should be taken to avoid overly forceful expansion, which can lead to issues with subsidence. After interbody graft placement is completed, pedicle screw fixation can then be performed in a similar fashion to the technique described in the tubular approach above.
Enabling Technologies
Advancements in surgical augmentation technologies have led to a natural integration with TLIF workflows to further optimize the scope of MIS-TLIF procedures. MIS-TLIF technology for the core elements of surgery—that is, surgical approach and hardware—begins with the variability of retractor systems and visualization modalities as described above. In addition to the standard tube, wide variations in retractor systems are available, including pedicle screw-based modular systems and tubular expandable retractors, which land along a spectrum on the balance between minimizing surgical imprint on surrounding tissues with providing more surgical site exposure. Many of these technologies incorporate variable arms that allow surgeons to directly control the degrees of freedom by which their operative corridor is visualized.
Though beyond the scope of this review, the permutations of different manners by which fusion may be done then extend across the full spectrum of possible alloy- and polymer-based interbodies, and an armamentarium of osteobiologics was intended for greater osteoinduction, osteoconduction, and osteogenesis. Advancements in the use of lordotic and expandable cages have allowed for a greater footprint to be achieved despite the smaller corridor by which MIS surgery functions. As part of this, the incorporation of novel modular screw systems may allow for greater flexibility in ipsilateral pedicle screw placement and ergonomics during interbody surgery.
Furthermore, additional advancements in image guidance, such as 3-D computed tomography–based navigation and augmented reality, can reduce surgeon radiation exposure and provide 3-D maps of the underlying anatomy. With improvements in accuracy and frameless stereotaxy, neuronavigation may allow for facilitated surgical efficiency and reduced rates of revision with potentially neutral-to-lower health care expenditures on malpositioned hardware.19–21 Moreover, the use of surgical robots may further the ability of surgeons to minimize tissue trauma and determine surgical plans upfront with reduced variability.22,23 The caveat to this remains the comfort level of the operator; improper technique and a lack of familiarity may obviate the theoretical advantages of navigation and present novel risks for surgeons unfamiliar with their workflows.
Many of these technologies offer the added advantage of improving surgeon ergonomics. With digital visualization methods, including camera-integrated retractors and endoscopy, surgeons can work around natural barriers to surgical field visualization that is inherent to any MIS technique. While many MIS advantages cater to patient-centric factors such as reduced blood loss and recovery times, the opportunity to avoid muscular stress and poor posture during surgery offers surgeons the ability to operate with comfort. As enabling technologies continue to grow and be applied to the MIS-TLIF, the procedure approaches a greater degree of personalization aimed at providing optimal fusion surgery for the correctly selected patient.
Anesthesia Considerations
Greater emphasis has been placed on the standardization of perioperative management, with a consensus statement on the implementation of enhanced recovery after surgery protocols in lumbar fusion presented in 2021 in order to reduce complications, shorten length of stay, and improve overall outcomes through targeted interventions.24 The supplementary use of local and regional anesthetic techniques was recommended in those guidelines to improve postoperative pain control. More recently, though, we have used conscious sedation in order to perform awake spinal fusion.18,25 As part of our protocol, a combination of long-acting liposomal bupivacaine for local anesthesia and a continuous ketamine-propofol sedative infusion is utilized to safely perform awake fusion surgery.26 When done as part of endoscopic MIS-TLIF, patients showed significant improvements in pain and disability at 1-year follow-up, often comparable to that of standard TLIF approaches.27 Notably, the awake anesthetic approach allows for direct and live patient feedback during potential DRG or nerve root irritation. The ability to perform MIS-TLIF under sedation can reduce the adverse effects of general anesthesia, including postoperative nausea and cognitive effects, and can reduce hospital length of stay. As a result, the ability to avoid general anesthesia and lengthy prone or open surgeries with greater surgical morbidity may improve the accessibility of TLIF surgery for patients in whom it may otherwise be a relative or absolute contraindication.
Outcomes of MIS-TLIF Approaches
Philosophically, the MIS-TLIF intends to minimize the muscle-stripping nature of open surgery via the use of native avascular corridors targeting the facet complex. Comparison of the cross-sectional tissue density in patients undergoing open and MIS surgery has shown reduced degrees of muscle breakdown in the latter.28,29 Moreover, cohort studies evaluating surgical morbidity have consistently demonstrated that open and MIS-TLIF approaches favor outcomes of MIS patients, specifically intra- and postoperative drainage, surgical blood loss, transfusion rates, and length of hospitalization.30,31 Evaluation of quality outcomes further demonstrates that patients report comparable rates of functional recovery in MIS techniques. Analysis of 297 patients within the Quality Outcomes Database registry has shown that 5-year outcomes for disability, back pain, leg pain, satisfaction, and quality of life did not differ across TLIF modalities when treating spondylolisthesis.32 Elsewhere, analysis has demonstrated reduced perioperative narcotic use with MIS techniques, with durable degrees of pain control at long-term follow-up and fusion rates exceeding 95%.33 MIS approaches demonstrate an opportunity for achieving the same outcomes as traditional open techniques but with the added utility of reducing operative morbidity.
Intuitively, the advantages of an MIS approach compared with open surgery may be drawn from a priori delineation of the relative workflows associated with each surgery. Greater nuance exists within defining the differences between various MIS modalities. Direct comparison between tubular and endoscopic approaches, as well as robot-assisted/percutaneous approaches, remains overall restricted to cohort analyses and, in the case of endoscopy, relatively shorter-term follow-up. However, on head-to-head comparison, modalities have not demonstrated significant variability to designate 1 MIS approach as “better” than another. Meta-analyses have demonstrated that endoscopic approaches often feature lower perioperative blood loss and short-term back pain recovery, likely from a smaller operative window, though long-term pain outcomes and complications do not vary markedly.34,35 Percutaneous and smaller working-channel techniques may present the advantage of reduced narcotic use compared with MIS techniques.36
Conclusion
The MIS-TLIF encompasses a diverse set of surgical techniques aimed at maximizing the footprint of achieving lumbar arthrodesis within a small corridor. Here, we present the technical considerations associated with tubular- and endoscopy-based systems. Fusion and symptom resolution outcomes in MIS-TLIF surgery rival those of traditional open TLIF procedures, but MIS-TLIF has the advantage of reduced procedural morbidity. With the growth of new technologies, variations of the MIS-TLIF continue to evolve. When framed in the context of patient-specific factors, this will enable surgeons to individualize treatment paradigms for optimal workflows and outcomes.
Acknowledgments
The authors contributed equally to this work and were involved in conceptualization, literature review, manuscript preparation, editing, and figure development.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosures Michael Y. Wang receives royalty payments from DePuy-Synthes Spine; is a consultant for DePuy-Synthes Spine, Inc., Stryker, Spineology, Surgalign, Pacira, and Nuvasive; and has stock in Innovative Surgical Devices, Kinesiometrics, and Medical Device Partners. Brian J. Park and Daivik B. Vyas have no disclosures to report.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2025 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.