


Abstract
Background A limited number of studies have compared the outcomes of anterior lumbar interbody fusion (ALIF) to transforaminal lumbar interbody fusion (TLIF) for the treatment of isthmic spondylolisthesis. This study aims to compare postoperative complications between these two surgical approaches.
Methods A retrospective review was performed using a large national database. The study population included all patients older than 18 years who underwent single-level ALIF or TLIF with a diagnosis of L5 to S1 isthmic spondylolisthesis. A 1:2 propensity score was used to match ALIF and TLIF cohorts for age, sex, and relevant comorbidities, including smoking status. Multivariate logistic regression was used to compare 3-month and 2-year medical and surgical complications, including 5-year reoperation rates.
Results Five hundred and seventy-eight ALIF patients were paired with 1,156 TLIF patients following the match. The analysis revealed a higher 3-month ileus rate in ALIF patients (P = 0.009) and a lower, though not significant difference in, reoperation rate for ALIF within 2 years at 7.1% compared with TLIF at 7.7% (P = 0.696). Five-year reoperation rates were comparable (9.5% vs 10.8%; P = 0.612).
Conclusions Aside from the increased rate of ileus in the ALIF group, there was no significant difference in both short- and mid-term complications, including overall reoperation rate, between the 2 techniques. Spine surgeons should select the optimal technique for a given patient.
Clinical Relevance ALIF and TLIF offer comparable mid-term postoperative outcomes for treating 1-level L5/S1 isthmic spondylolisthesis.
Level of Evidence 3.
Introduction
Isthmic spondylolisthesis is defined as the anterior translation of 1 vertebra relative to the next caudal segment as a result of the pars defect.1 Mild isthmic spondylolisthesis is often asymptomatic, but as the condition progresses, it gradually leads to intervertebral instability and foraminal stenosis, giving rise to lower back pain and radicular symptoms. This slippage most commonly occurs at L5 to S1, followed by L4 to L5. The incidence of isthmic spondylolisthesis in patients aged 40 to 80 years with symptoms of low back pain is estimated at 8.2%.2 As the degree of spondylolisthesis worsens, it leads to L5 to S1 foraminal stenosis, thereby compressing the exiting L5 nerve root or tension of the traversing S1 nerve root.3 Patients with unilateral spondylolysis usually do not develop spondylolisthesis, but 40% to 66% of patients with bilateral spondylolysis will develop spondylolisthesis.1 Lumbar lordosis in the normal spine is mainly caused by the lower lumbar segment.4 In isthmic spondylolisthesis, symptoms may be precipitated by sagittal imbalance leading to muscle pain in the lower back. Restoring segmental lordosis at L5 to S1 and L4 to L5, the segments with the highest lordosis, is a key principle in maintaining alignment within the normal range and avoiding the compensatory mechanisms that lead to disability.5
When nonoperative medical and functional strategies prove inadequate, surgery may be required. Interbody fusion now seems the most widely recommended strategy,6 whether approached anteriorly or posteriorly.7,8 Regardless of which technique is chosen, the goals are the same: release the neurological structures, stabilize the vertebral slippage, and restore disc height and physiological segmental lordosis. Meanwhile, various techniques are available, and consensus is hard to reach.9,10 Thus, although L5 to S1 isthmic spondylolistheses are commonly treated with either anterior lumbar interbody fusion (ALIF) or transforaminal lumbar interbody fusion (TLIF),9,11 there is a paucity of evidence-based consensus on clinical and radiographic outcomes and, as a result, on technical superiority.
While a significant body of literature exists on the subject of L5 to S1 isthmic spondylolisthesis, only a handful of studies have directly compared the outcomes of different techniques involving instrumentation and interbody grafting for its treatment. Additionally, there appears to be a lack of consensus on which approach is associated with superior outcomes. This study’s primary objective was to perform a comparative analysis of the outcomes between TLIF and ALIF for the surgical treatment of L5 to S1 isthmic spondylolisthesis.
Methods
Data Source
The data used in this analysis were obtained from the multipayer database PearlDiver (PearlDiver Inc., Colorado Springs, Colorado, USA), which contains records of more than 161 million patients. These data included procedural and demographic information encoded with International Classification of Diseases (ICD) and Current Procedural Terminology (CPT) codes. In full compliance with the Health Insurance Portability and Accountability Act, all data are deidentified.
Study Population
Adult patients with L5 to S1 isthmic spondylolisthesis included in this study were identified from ICD codes defining lumbosacral region spondylolisthesis (ICD-10-D-M4317) and lumbosacral region spondylolysis (ICD-10-D-M4307) from 2015 to 2020Q1 (quarter 1). Patients with active or prior history of malignancy, trauma, or infection were excluded. Two separate cohorts were created based on the surgical technique: ALIF with posterior instrumentation (CPT-22558 and CPT-22612) and TLIF (CPT-22633). Multilevel ALIF and TLIF (CPT-22585 and CPT-22634) were excluded. All patients had a minimum of 2-year follow-up.
Propensity score matching for 2 groups was performed with a 1:2 ratio based on age, sex, and baseline comorbidities including Charlson Comorbidity Index (CCI), obesity, morbid obesity, smoking status, chronic pulmonary disease, peripheral vascular disease, diabetes mellitus, hyperlipidemia, hypertension, hypothyroidism, congestive heart failure, coronary artery disease, depression, rheumatoid arthritis, and osteoporosis. Data on the use of access surgeons and bone grafts (allografts and bone morphogenetic protein [BMP]) during the surgical procedures were also collected.
Outcomes
Three-month medical complications included arrhythmia, myocardial infarction, cardiac arrest, atelectasis, respiratory failure, pleural effusion, pulmonary embolism, deep vein thrombosis, cardiovascular accident, delirium, ileus, bowel obstruction, electrolyte abnormality, renal failure, urinary retention, pneumonia, sepsis, and urinary tract infection. Three-month surgical complications included dural tear, nerve root injury, vascular injury, visceral injury, transfusion, motor/sensory deficit, radiculopathy, spinal cord deficit, cauda equina deficit, wound dehiscence, seroma, hematoma, deep wound infection, and superficial wound infection. Two-year complications included instrumentation failure, pseudarthrosis, vertebral body fracture, and reoperation.
Statistical Analysis
Pearson χ 2 test was used to assess for differences in demographics and pre-existing comorbidities. Welch’s t test was used to assess for differences in mean age and CCI. Multivariable logistic regression was used to determine the independent effects of the surgical technique on the postoperative outcomes after adjusting for demographic factors and pertinent comorbidities. Kaplan–Meier survival plots were produced for 5-year revision and compared through log-rank test. All statistical analyses were conducted using the research query interface provided by PearlDiver Bellwether. The common statistical metrics, including frequencies, mean values, and odds ratios, were collected by the Bellwether system using the R statistical package. Statistical significance was set at P < 0.05.
Results
Upon applying exclusion criteria and 1:2 propensity matching, 578 ALIF patients were matched with 1156 TLIF patients. The mean age of patients was 48.9 ± 13.1 years in the ALIF group and 49.1 ± 12.8 years in the TLIF group (P = 0.847). Gender distribution also did not differ significantly between the 2 groups, with women constituting 56.3% of the ALIF group and 51.4% of the TLIF group (P = 0.087). Comorbidities were assessed using the CCI, with both groups having a mean score of 1.3 ± 1.6 (P = 0.521). Other chronic comorbid conditions were similar between the 2 groups, with no significant differences noted. An access surgeon was used in 37.2% of ALIF cases. In terms of bone grafting, BMP was used more frequently in the ALIF group compared with the TLIF group (9.0% vs 4.3%, P < 0.001; Table 1).
Clinical characteristics of 1734 patients undergoing surgical treatment for L5 to S1 isthmic spondylolisthesis with minimum of 2-year follow-up.
In the gastrointestinal category, a significant difference was noted in the occurrence of ileus within 3 months postoperation, with patients undergoing ALIF experiencing a higher incidence compared with those receiving TLIF (2.1% vs 0.5%; OR 4.31, 95% CI 1.50–14.13; P = 0.009). The total number of medical complications and the number of patients affected by any complication were similar between the groups (P = 0.923; P = 0.696; Table 2).
Multivariate analysis of rates of 90-day medical complications by category for both groups.
There were no significant differences in operative, neurological, wound/infectious, and implant-related complications, and reoperation rate was slightly lower in the ALIF group at 7.1% compared with the TLIF group at 7.7%, though there was no significant difference (P = 0.696). The total number of surgical complications and the number of patients affected by any surgical complication were compared, and again, no significant difference was found between the 2 groups (P = 0.671; P = 0.170; Table 3).
Multivariate analysis of rates of 90-day and 2-year surgical complications by category for both groups.
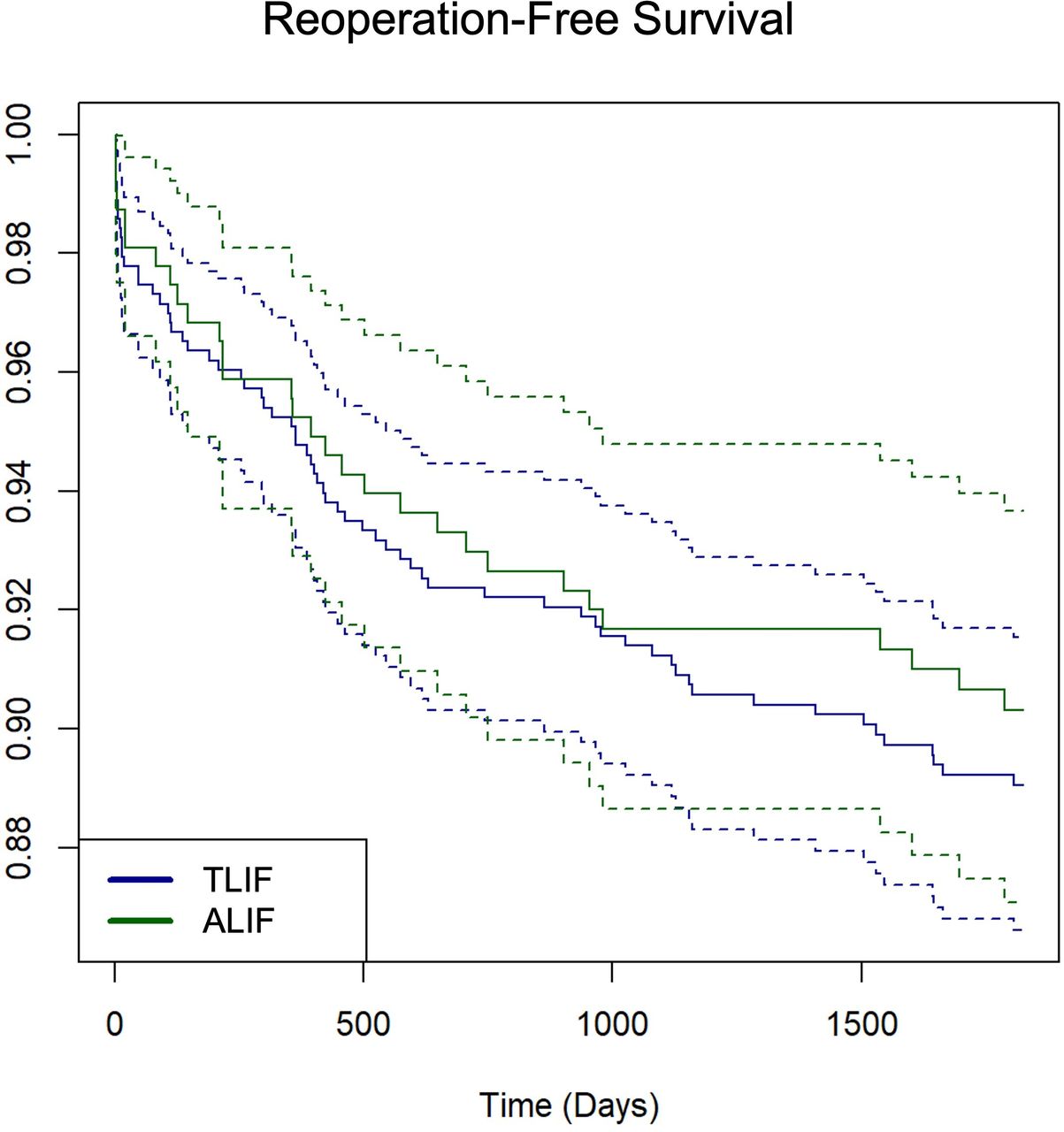
During the 5-year follow-up, there were 316 patients left in the dataset in the ALIF group and 632 patients in the TLIF group. There was a lack of statistical significance in reoperation rate with 30 patients (9.5%) needing surgical reintervention in the ALIF group and 68 patients (10.8%) in the TLIF group needing reoperation (P = 0.612). Dotted lines indicate 95% confidence intervals (Figure).

Kaplan–Meier plot showing 5-year reoperation-free survival following surgical management of L5 to S1 isthmic spondylolisthesis (P = 0.612). Dotted lines indicate 95% confidence interval.
Discussion
Multiple surgical approaches have been devised to treat isthmic spondylolisthesis; however, a definitive consensus on the optimal technique remains elusive. ALIF and TLIF stand out as the most commonly used techniques utilized for addressing isthmic spondylolisthesis, with each technique carrying distinct risks and benefits. ALIF may be performed as a stand-alone procedure or in combination with a posterior pedicle screw construct. However, performing ALIF alone increases the risk of instrument failure.12 In the context of isthmic spondylolisthesis, our goal is to restore the spine’s proper alignment and rebuild lumbar stability. Therefore, ALIF with posterior instrumentation creates circumferential fixation, thus enhancing stability and promoting interbody fusion. On the other hand, TLIF techniques require dissection of the paravertebral lumbar musculature, with insufficient exposure of the intervertebral disc and inadequate correction of lumbar lordosis. Furthermore, there is a higher risk of dural tears or cerebrospinal fluid leakage.9,13,14 The primary objective of the present study was to compare the medical and surgical complications of ALIF and TLIF treatments for L5 to S1 isthmic spondylolisthesis.
Many sources suggest that ALIF is associated with a higher incidence of deep vein thrombosis, gastrointestinal complications, and anemia, even with a 1.5 times higher mortality rate compared with posterior approaches.15,16 During anterior approach surgery, there are varying degrees of disruption to the abdominal tissues when exposing the surgical field. The traditional method for performing ALIF involves placing the patient in a supine position while using an inflated back cushion to enhance the lumbar lordosis. The procedure is carried out through a retroperitoneal approach. Although ALIF approaches offer wider access to the disk space, the dissection involves considerable potential risks due to the exposure of major vessels, ureter, organs, and the hypogastric plexus. Our data confirmed that there is an increased occurrence of ileus in the ALIF group. A retrospective database analysis conducted by Fineberg et al reported an increased incidence of postoperative ileus with anterior approaches for lumbar fusion.17 Beyond that, the incidence rates of complications, such as pneumonia, deep vein thrombosis, pulmonary embolism, sepsis, and others, were not significantly different between ALIF and TLIF. Additionally, the incidence rates of cerebrovascular accidents, delirium, and myocardial infarctions also did not demonstrate significant differences.
The 2013 North American Spine Society guidelines on the diagnosis and treatment of isthmic spondylolisthesis indicated that there was currently insufficient evidence to suggest which surgical approach is more advantageous for improving long-term prognosis in adult patients undergoing surgical treatment. So far, several large-scale retrospective reviews and meta-analyses have emphasized the respective complication characteristics of anterior and posterior surgical approaches, with no significant differences in terms of reoperation rates, nerve root injuries, and infection rates.16–19 There are also differing findings. Alhammoud et al, through a meta-analysis, arrived at results showing a higher incidence of surgical site infections, dural injuries, and implant misplacements in posterior approach surgeries.20 Phan et al also demonstrated that TLIF carries a higher risk of dural tear or cerebrospinal fluid leakage.13 However, our results indicated that there were no clear differences in rates of infection, nerve root injury, dural tear, or wound complications.
Alhammoud et al also found that there was no significant difference in fusion rate between ALIF and TLIF approaches.20 Alhauge et al found no significant difference in reoperation rates between ALIF and TLIF for isthmic spondylolisthesis,21 consistent with our findings. However, they noted that the subgroup sample was too small to yield statistically robust conclusion. Nevertheless, according to the clinical guidelines on isthmic spondylolisthesis from the North American Spine Society, circumferential fusion has been identified as capable of improving clinical outcomes in adult patients and achieving higher radiographic fusion rates.1 At the same time, there is also a large amount of literature showing that for the restoration of lumbar lordosis, ALIF is superior to TLIF.13,14,22,23 Nonetheless, Prost et al concluded that ALIF provides faster relief of postoperative low back pain than TLIF, but there are no significant clinical differences between techniques. Despite better restoration of disc height and lumbar lordosis in the ALIF group, there was no difference in the restoration of global lordosis.9 Similarly, Thompson et al also found similar long-term reductions in pain and functional disability between ALIF and TLIF. Additionally, they noted that ALIF patients experienced faster reductions in pain and disability within 1 year.24
While some literature has shown strong evidence that ALIF and TLIF have similar rates of reoperation,18,19 other reviews demonstrated that TLIF has a higher reoperation rate compared with ALIF.7,20 This reason could be due to the bigger footprint of ALIF cages, resulting in greater stability, hence leading to fewer instances of internal fixation failure. However, in our study, no significant differences were found in terms of reoperation rate and instrument failure rate. The reoperation rate mainly depends on instrumentation failure and pseudarthrosis. This is likely explained by the fact that both techniques involve anterior column support using interbody cages, as well as posterior stability with pedicle screws, resulting in similar circumferential biomechanical stability. Javernick et al discovered that in TLIF, a unilateral transforaminal approach can remove around 69% of disc volume, while a bilateral approach can remove approximately 80% of the volume.25 They concluded that the removal of disc material through unilateral TLIF was sufficient to achieve a solid and stable joint fusion while minimizing neural retraction and dural exposure. The similar reoperation rates between TLIF and ALIF may be attributed to TLIF having sufficient biomechanical stability and removing an adequate volume of intervertebral disc material.
One important consideration when selecting between ALIF and TLIF is cost. ALIF has been shown to be associated with higher costs compared with posterior fusion alone,16,26 primarily due to longer operative times, the need for changing patient positions during surgery, and the increased cost of implants and BMP usage. Moreover, ALIF often requires coordination with an access surgeon, which can lead to scheduling challenges and potential delays, further increasing resource utilization. These additional costs contribute to a higher overall financial burden. While ALIF may offer superior outcomes in specific cases, the increased resource utilization should be carefully considered in the context of patient care and healthcare economics. Future research should continue to investigate strategies for reducing these costs without compromising patient outcomes, particularly in healthcare systems where resource allocation is critical.
This study leverages the strength of large national databases, enabling the examination of rare conditions on a grand scale, which is a challenge for single institutions. With 1656 patients, our study avoids the pitfalls of small sample sizes and regional biases common in single-center studies. The PearlDiver database stands out with its capability to track postoperative patient data longitudinally, unlike databases like the National Inpatient Sample and National Surgical Quality Improvement Program, which can only monitor complications occurring during the hospital stay or within 30 days postsurgery. These extensive data offer a reliable source of both short and mid-term outcomes, making it a valuable reference for surgeons and patients evaluating surgical treatments for isthmic spondylolisthesis.
Unfortunately, the use of a large retrospective database has inherent limitations. The study’s reliability hinges on the precision of database coding, and though human error might lead to coding inaccuracies, it is estimated to affect only about 1.1% of all entries.27 Our comprehensive multivariate regression analysis helps mitigate some coding-related biases. Still, it cannot account for variables outside the database, such as operative time, blood loss, minimally invasive vs traditional open spine surgery, use of hyperlordotic cage, and most importantly classification/grade of isthmic spondylolisthesis, which might influence the results. Furthermore, radiographical and patient-reported outcomes could not be assessed due to the nature of nongranularity of the database, and those could have provided additional insights into the course of development of complications, including nonsignificance in reoperation rate. It is important to recognize that both techniques are essential to the development of the surgical treatments of lumbar pathologies, with each offering unique advantages and disadvantages. Therefore, the spine surgeon should choose the superior technique based on patient-specific factors; clinical judgment should encompass a patient’s unique anatomy as well as certain medical comorbidities/history that might further predispose a patient to surgical complications such as ileus.
Conclusion
The current study represents the largest comparative study examining postoperative outcomes following ALIF and TLIF for the treatment of L5 to S1 isthmic spondylolisthesis. Our analysis supports that ileus is more likely to occur in the ALIF approach compared with TLIF. However, there were no statistically significant differences in other operative, neurological, wound/infectious, and implant-related complications, as well as reoperation rates within 5 years. In order to elucidate possible advantages of ALIF vs TLIF, future research should further stratify the comparative groups by variables outside the database, notably the grade of isthmic spondylolisthesis. These data, although compelling, must be interpreted in the context of a large dataset that lacks certain granularity.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2025 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.