


Abstract
Background Patients often undergo circumferential (anterior and posterior) spinal fusions to maximize adult spinal deformity (ASD) correction and achieve adequate fusion. Currently, such procedures are performed in staged (ST) or same-day (SD) procedures with limited evidence to support either strategy. This study aims to compare perioperative outcomes and costs of ST vs SD circumferential ASD corrective surgeries.
Methods This is a retrospective review of patients undergoing circumferential ASD surgeries between 2013 and 2018 in a single institution. Patient characteristics, preoperative comorbidities, surgical details, perioperative complications, readmissions, total hospital admission costs, and 90-day postoperative care costs were identified. All variables were tested for differences between ST and SD groups unadjusted and after applying inverse probability weighting (IPW), and the results before and after IPW were compared.
Results The entire cohort included a total of 211 (ST = 50, SD = 161) patients, 100 of whom (ST = 44, SD = 56) underwent more than 4 levels fused posteriorly and anterior lumbar interbody fusion (ALIF). Although patient characteristics and comorbidities were not dissimilar between the ST and SD groups, both the number of levels fused in ALIF and posterior spinal fusion (PSF) were significantly different. Thus, using IPW, we were able to minimize the cohort incongruities in the number of levels fused in ALIF and PSF while maintaining comparable patient characteristics. In both the whole cohort and the long segment fusions, postoperative pulmonary embolism was more common in ST procedures. After adjustment utilizing IPW, both groups were not significantly different in disposition, 30-day readmissions, and reoperations. However, within the whole cohort and the long segment fusion cohort, the ST group continued to show significantly increased rates of pulmonary embolism, longer length of stay, and higher hospital admission costs compared with the SD group.
Conclusions Adjusted comparisons between ST and SD groups showed staging associated with significantly increased length of stay, risk of pulmonary embolism, and admission costs.
Level of Evidence 2.
Introduction
As the global population witnesses a shift in its age distribution and instrumented spine surgery becomes more commonplace, adult spinal deformity (ASD) has become increasingly prevalent, resulting in greater utilization of corrective surgeries to achieve definitive management.1–4 ASD includes a spectrum of spinal pathologies that can lead to many debilitating morbidities and ultimately poor quality of life.2–5 Management of ASDs can be challenging, including identifying the nuances of each deformity profile, as well as determining the optimal treatment plan, which can range from nonoperative management to long-segment surgical corrections.6,7 The utilization of these spinal fusions and instrumentation for ASD treatment has grown exponentially over the past 2 decades as a result of improvements in the understanding of spinal deformity along with advancements in technological resources and surgical techniques.8 This has been especially true in elderly patients as the use of long fusion constructs in this population increased 460% from 2004 to 2015.8 With this significant rise in ASD surgery, surgical morbidity and outcomes have also increased.9,10
Due to procedural length and technical complexities, one of the decisions surgeons often make when planning multiapproach corrective surgeries for ASD (ie, anterior, posterior, lateral, or a combination) is whether or not to stage the procedure. There is a paucity of literature covering staged (ST) ASD procedures due to the unique considerations for each case.3,11–14 Some surgeons prefer to perform each approach separately as, in theory, this should minimize the morbidity of complex spine surgery related to the duration of the surgery, especially when many patients are elderly with associated comorbidities. Other surgeons favor combining approaches into same-day (SD) surgery. This school of thought aims to reduce the total operative time, blood loss, and use of anesthesia, as well as the medical complications associated with lengthy hospital stays. SD procedures may also help decrease the high cost of ASD surgery and theoretically shorten hospital stay. The significant complexity associated with ASD corrective surgeries, as well as the comorbidities often associated with the patient population, tends to raise health care costs per episode of care.12 Indeed, hospital costs for elective lumbar spinal fusions surpassed the margin of $10 billion in 2015, while the mean cost per admission exceeded $50,000.15
While differences between performing ASD procedures on the SD or in an ST manner are modestly covered, the available literature has many limitations. The studies rely on small samples, making recommendations difficult to interpret.16,17 To combat this, some studies include diverse pathologies such as neoplastic, infectious, or traumatic causes requiring complex spine surgery. However, this results in data that cannot be used to guide treatments for specific populations.12,18
The purpose of the present study is to analyze the differences in intraoperative and postoperative complication profiles, length of stay (LOS), readmission rates, discharge dispositions, and costs of ST and SD complex corrective surgeries in ASD patients after accounting for preoperative and surgical variations, including a subgroup analysis of patients undergoing correction involving more than 4 spinal levels.
Methods
Data Source
This study is a retrospective review of a single institution’s electronic medical records of patients with ASD-related pathologies who underwent ASD corrective surgeries between 2013 and 2018. Inclusion criteria for this study included age >18 years at the time of surgery and diagnoses of ASD (ie, flatback syndrome, spondylolisthesis, degenerative disc disease, scoliosis, kyphoscoliosis, and failed back syndrome) and undergoing combined anterior lumbar interbody fusion (ALIF) and open posterior lumbar or thoracolumbar instrumented spinal fusion (posterior spinal fusion [PSF]). Exclusion criteria included patients undergoing spine surgery for treatment of neoplastic, traumatic, or infection-related diagnoses or patients undergoing interbody fusion procedures using any approach that was not an open ALIF.
Study Design
The patient cohort was divided into 2 groups: ST or SD. Only patients who received ST procedures (2 separate visits to the OR with 2 separate anesthesia events) during the same admission were included in the study; patients who received ST procedures on separate admission encounters were excluded. SD patient group underwent ALIF and PSF procedures on the same day in a single visit to the OR with one anesthesia event.
Data Collection
The data utilized in the study included patients’ demographics, characteristics, preoperative comorbidity diagnoses, surgical details, intraoperative complications (including durotomy, vascular injury, neuromonitoring deterioration, hypovolemic shock, ST elevation, or respiratory compromise), postoperative complications (including acute blood loss, deep venous thrombosis/pulmonary embolism [DVT/PE], altered mental status, arrhythmias, fever/bacteremia, transient ischemic attack or strokes, respiratory distress, hematoma, surgical site infection, and instrument-related complications), readmissions, reoperations, disposition, and LOS. Additionally, total hospital admission costs and postoperative 90-day cost of care were included when available.
Statistical Analysis
All patient demographics, preoperative comorbidities, surgical details, postoperative complications, LOS, cost, readmission, and reoperations were assessed unadjusted and after inverse probability weighting (IPW). The methods utilized allowed for comparisons between the unadjusted and IPW results while remaining appropriate in isolation. This approach was used for the entire cohort and a subgroup of patients, including only those undergoing 4 or more levels of posterior fusion.
Unadjusted
Normality was assessed for continuous variables through a Shapiro Wilk’s test and visual inspection of the histogram and quantile-quantile plot. For variables that were approximately normal, t tests were performed on the differences between ST and SD groups; the mean differences and their 95% CIs were reported. For variables significantly non-normal, a log transformation was applied, and for each log outcome, 1-way analyses of variance were run; normality of the residuals were tested, and the mean ratios of ST to SD with their 95% CIs were reported. For the categorical variables, Fisher’s exact tests were used to identify any significant associations between both groups, and the odds ratios with their exact 95% CIs were reported.
Inverse Probability Weighting
To control for patient characteristics and comorbidity differences between the ST and SD groups, we created a pseudoexperiment with IPW. It was essential that there was no evidence of a dissimilar number of levels fused in ALIF and the number of levels fused in PSF between cohorts while simultaneously minimizing differences in patient characteristics and comorbidities. Due to sample size restrictions, we were unable to weight base all patient demographics, comorbidities, and surgical details. For the full cohort, our weighting variables included race, sex, smoking status, number of levels fused in ALIF, and number of levels fused in PSF, while for the 4+ number of levels fused in PSF, our weighting variables included body mass index (BMI), preoperative American Society of Anesthesiologists (ASA), number of levels fused in ALIF, and number of levels fused in PSF. These variable selections minimized differences in the ST and SD groups in their respective analyses.
For continuous outcomes, 1-way analyses of variance with the probability weights were constructed, and the residuals were assessed. If the residuals were approximately normal, the mean differences and their 95% CIs were reported. If the residuals were significantly non-normal, log transformations were applied to the outcome, and normality of the residuals were reassessed; the mean ratios of ST to SD with their 95% CIs were reported. For binary variables, univariate logistic regressions with the probability weights included were fit, and the odds ratios with their 95% Wald CIs were reported. All statistical analyses were performed using Stata version 17.0.
Results
Univariate Analysis and IPW
Patient Population
Whole Cohort
A total of 211 patients (ST = 50, SD = 161) were included in this analysis. There was no significant difference in age and sex distribution, mean BMI, and smoking status between the groups. The racial distribution was significantly different between both groups, with significantly more White patients in the ST group. However, after IPW, the differences in race were no longer seen (Table 1).
Preoperative characteristics for the whole cohort.
Long Segment (LS) Cohort
Within the subgroup of 100 patients who underwent fusion of more than 4 levels (ST = 44, SD = 56), the ST and SD groups were not significantly different in terms of demographics, including age, sex, mean BMI, smoking status, and race (Table 2).
Preoperative characteristics for the long segment cohort.
Preoperative Comorbidities
Whole Cohort
Both surgical groups were not significantly different in the incidence of diabetes mellitus, history of PE/DVT, hyperlipidemia, hypertension, ischemic heart disease, other cardiovascular comorbidities, anemia, coagulation disorders, mood disorders, other psychiatric comorbidities, thyroid disorders, and postmenopausal osteoporosis defined as a bone marrow density T-score −2.5 or less, preoperative ASA grades, and chronic obstructive pulmonary disease (COPD) in the unadjusted analysis. In the IPW model, patients undergoing ST procedures had a significantly higher rate of COPD (OR = 8.6, P = 0.006), a necessary sacrifice to ensure nonsignificantly different levels fused ALIF and PSF (Table 1).
LS Cohort
The association between ST procedures and COPD was not seen in the cohort of patients who underwent more than 4 levels of fusion. In this subgroup, all other comorbidities as listed above were not significantly different with unadjusted or IPW analyses (Table 2).
Surgical Details
Whole Cohort
As expected, univariate comparison of both surgical groups showed significantly more levels fused for the ST vs the SD group. ST group underwent a significantly higher number of levels fused via ALIF than in the SD group (74% with 2 or more levels fused vs 48%, P < 0.001). We observed a higher mean number of levels fused via PSF for the ST group than the SD group, and the expected number of levels fused in PSF for the ST group is 2.8 times greater than the SD group (P < 0.001). We observed higher mean combined estimated blood loss ST group than the SD group, and the expected combined estimated blood loss (EBL) for the ST group is 2.3 times greater than the SD group (P < 0.001). With IPW, the significant differences between the ST and SD groups with respect to number of levels were not recapitulated, indicating that IPW was able to control for this difference in analysis. The median duration between ST procedures was 2.9 days with a range of 0 to 22 days (Table 3).
Perioperative characteristics
LS Cohort
For patients undergoing more than 4 levels of fusion, the number of levels fused anteriorly was significantly higher in ST procedures on unadjusted analysis (75% with 2 or more levels fused vs 39%, P < 0.001). We observed a higher mean number of levels fused via PSF for the ST group than the SD group (mean = 10 vs 7.3), and the expected number of levels fused in PSF for the ST group was 1.4 times greater than it was for the SD group (P < 0.001). These differences were not seen on IPW analysis. In those undergoing more than 4 levels of fusion, EBL averaged 1224.9 mL, and the expected ratio of combined EBL between SD and ST was not significantly different between ST and SD groups on either unadjusted or IPW analysis. The median duration between ST procedures was 2.9 days with a range of 0–22 days for the LS cohorts (Table 3).
Perioperative Complications
Whole Cohort
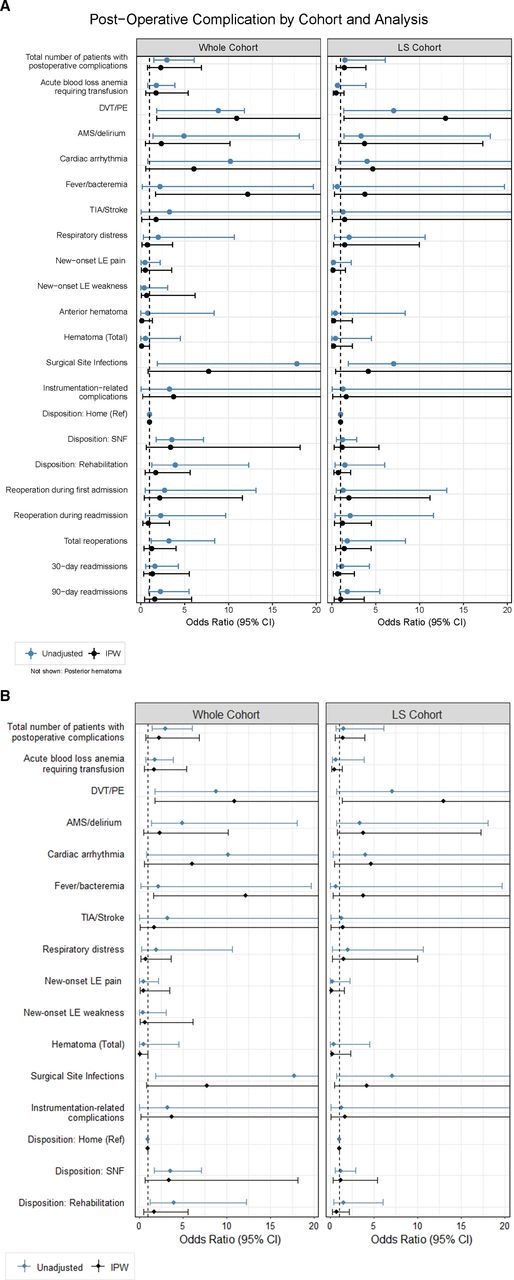
Intraoperative complications were recorded in 11 cases (5.2%), and the ST group showed a significantly higher incidence compared with the SD group (OR = 6.4, P = 0.004). The total number of patients with postoperative complications was 88 (41.7%; Table 3). Similarly, the ST group showed a significantly higher number of patients with postoperative complications compared with the SD group in the univariate analysis (OR 2.97, P = 0.001). Additionally, the ST group had a significantly higher incidence of postoperative PE, altered mental status or delirium, cardiac arrhythmia, and surgical site infections. Both groups were similar in the rates of postoperative fever/bacteremia, respiratory distress, new-onset lower extremity (LE) pain or weakness, the development of wound-related hematoma anteriorly, posteriorly, or in total, and instrumentation-related complications (Figure 1). Using IPW, the rate of postoperative PE remained significantly higher in ST vs SD (12% vs 1.2%, P = 0.045; Figure 2), and unlike in the unadjusted analysis, the odds of fever/bacteremia were significantly higher for the ST group (OR = 12.2, P = 0.014), while the odds of total hematoma were significantly lower for the ST group (OR = 0.1008, P = 0.049; Table 4).

Postoperative complications. In the whole cohort, the staged (ST) group had more complications compared with the same-day (SD) group in the univariate analysis (OR 2.97, P = 0.001) and significantly higher incidence of postoperative pulmonary embolism (PE), altered mental status or delirium, cardiac arrhythmia, and surgical site infections. There were 63 patients (63%) with a postoperative complication within the long segment cohort with no difference between ST and SD groups on unadjusted analysis. Abbreviations: AMS, altered mental status; DVT, deep venous thrombosis; IPW, inverse probability weighting; LE, lower extremity; LS, long segment; PE, pulmonary embolism; SNF, skilled nursing facility; TIA, transient ischemic attack.

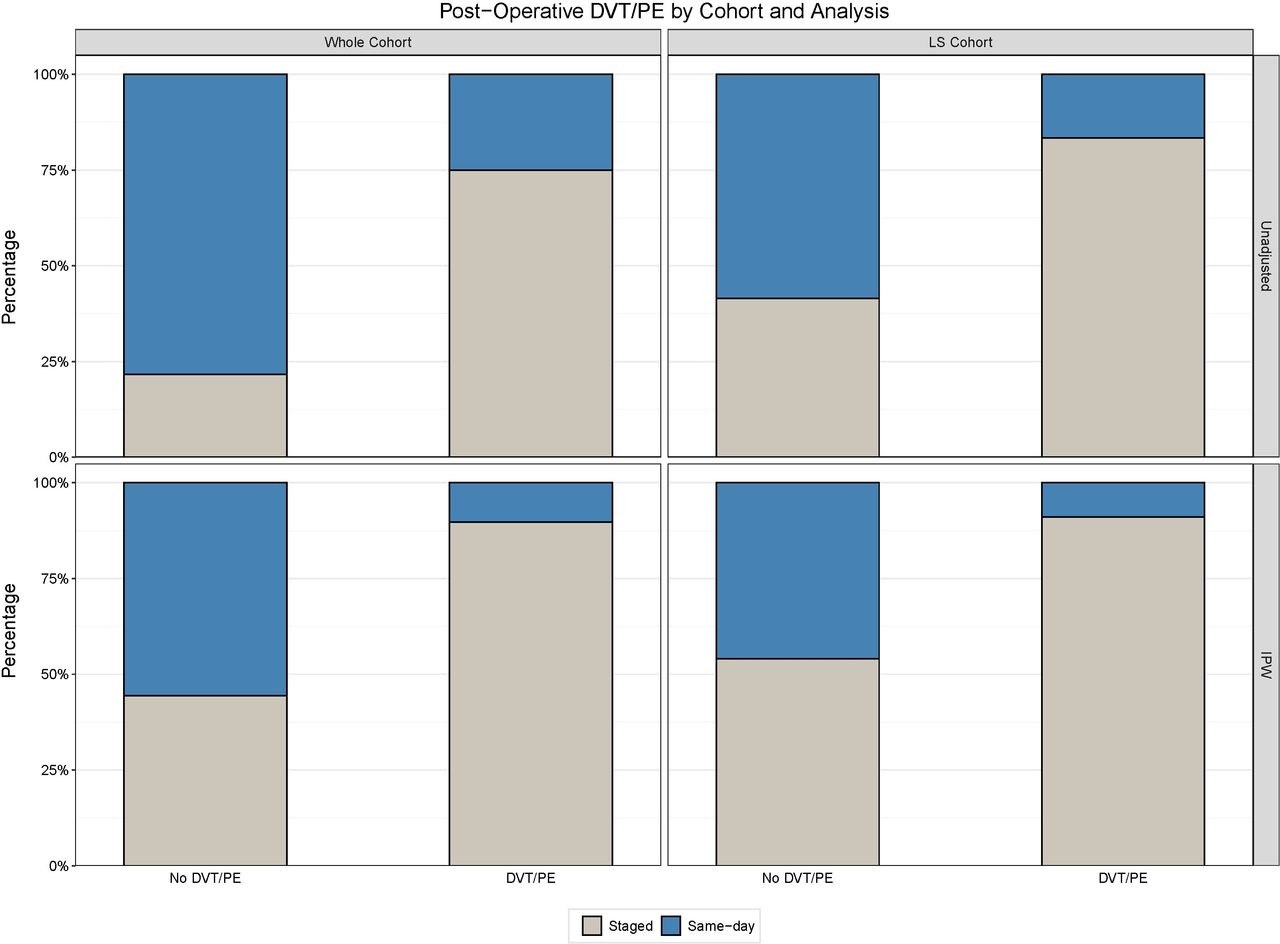
Postoperative PE. Using IPW, the rate of PE was significantly higher in staged (ST) vs same-day (SD) groups in the whole cohort (12% vs 1.2%, P = 0.045). In the long segment cohort, there was a significant difference in the rate of postoperative PE in the ST vs SD group (OR = 13.0, P = 0.24). Abbreviations: DVT, deep venous thrombosis; IPW, inverse probability weighting; LS, long segment; PE, pulmonary embolism.
Postoperative characteristics.
LS Cohort
Intraoperative complications were recorded in 8 patients (8%) with no statistically significant difference between ST and SD groups (Table 3). There were 63 patients (63%) with a postoperative complication within the LS cohort with no difference between the ST and SD groups on unadjusted analysis (Table 4; Figure 1). However, IPW showed a significant difference in the rate of postoperative PE in the ST vs SD groups (OR = 12.96, P = 0.025; Figure 2).
LOS and Disposition
Whole Cohort
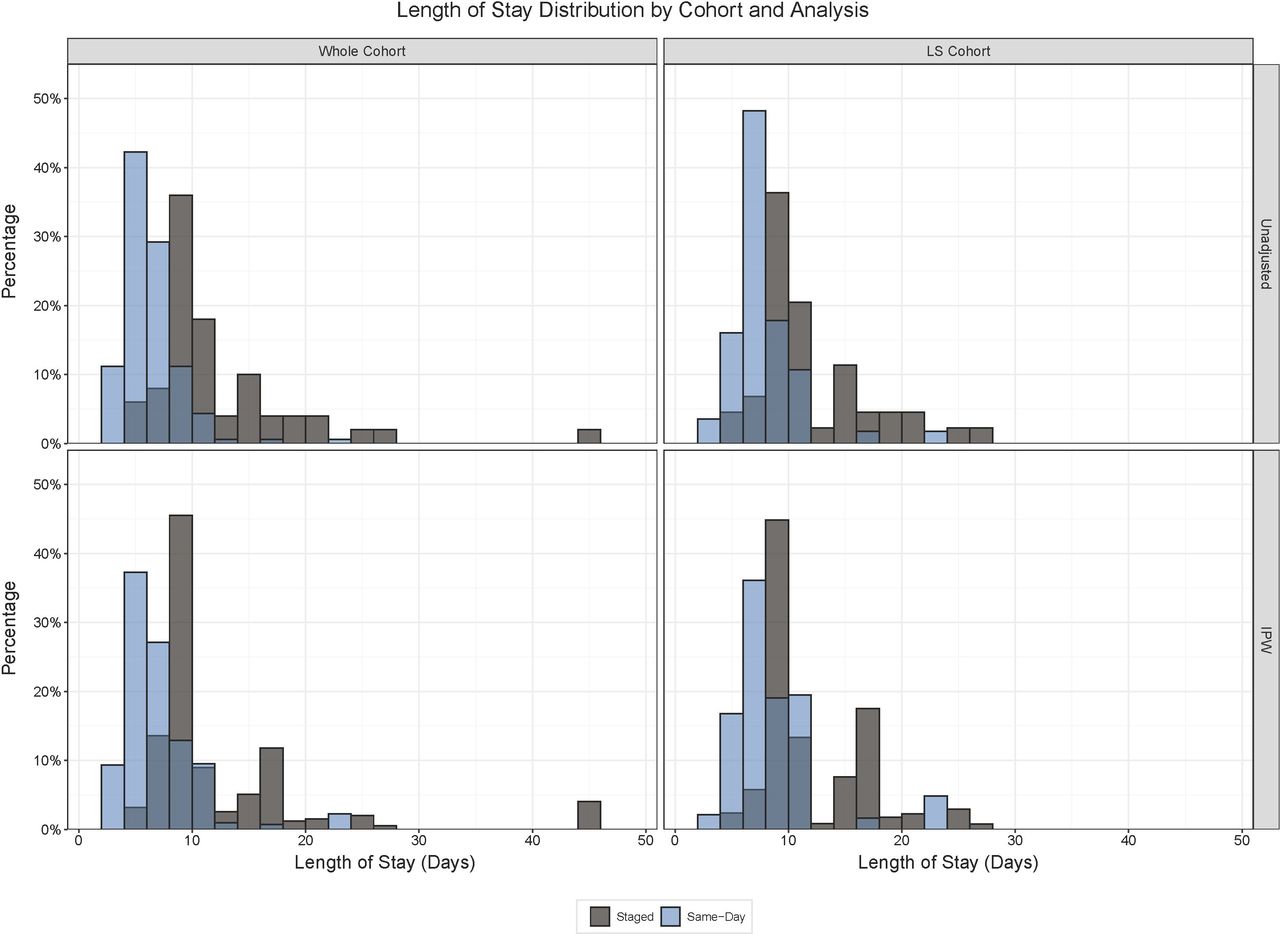
In both unadjusted and IPW analyses, we observed a longer LOS for the ST group than for the SD group (10.8 vs 4.8 days), and the ST group was expected to have LOS 2.2 times longer than the SD group (P < 0.001; Figure 3). The disposition of patients in the total cohort after discharge was also significantly different as the ST group showed a greater number of discharges to a skilled nursing facility (SNF) or inpatient rehabilitation (60% vs 30.4%, P < 0.001). With IPW, the discharge disposition was no longer statistically significant, but LOS was similarly significant (Table 5).

Length of Stay: In both unadjusted and IPW analyses, the length of stay for the staged (ST) group was longer than the same-day (SD) group (10.8 vs 64.8 days), and the ST group was expected to have length of stay 2.2 times longer than the SD group (P < 0.0001) in the whole cohort. In the long segment cohort, on both unadjusted and IPW analyses, we observed a longer length of stay for the ST group than the SD group (10.5 vs 6.2 days), and the ST group was expected to have length of stay 1.7 times longer than the SD group (P < 0.0001). Abbreviations: IPW, inverse probability weighting; LS, long segment.
Length of stay and readmissions.
LS Cohort
In both unadjusted and IPW analyses, we observed a longer length of stay for the ST group than for the SD group (10.5 days vs 6.2 days), and the ST group was expected to have length of stay 1.7 times longer than the SD group (P < 0.001) (Figure 3). There was no significant difference in discharge disposition. One patient in the ST group undergoing fusion of more than 4 levels died during primary hospitalization on postoperative day 6 after becoming bradycardic and requiring multiple rounds of cardiopulmonary resuscitation for pulseless electrical activity (Table 5).
Reoperations and Readmissions
Whole Cohort
The total 30-day readmission in the study’s cohort was 25 (11.8%), while 29 (13.7%) 90-day readmissions were recorded. Thirty- and 90-day readmission rates were similar in both groups. The rate of reoperations during the index surgery admission was not significantly different between groups. However, total reoperations, including reoperations on readmissions, were significantly higher in the ST group (P = 0.011), though this difference was not seen using IPW (Table 5).
LS Cohort
There was no significant difference in the unadjusted or IPW analyses of 30- (15.9% vs 14.3%) and 90-day (22.7% vs 14.3%) readmission rates in patients undergoing more than 4 levels of fusion between ST or SD groups. Reoperations did not significantly differ between groups within this cohort (Table 5).
Hospital Cost Analysis
Whole Cohort
We observed the mean cost for SD patients was $71,193 compared with $145,907 for ST patients. For the unadjusted analysis, the average cost was 1.9 times greater in the ST group vs the SD group (95% CI 1.6008, 2.2698, P < 0.001). This was also seen with IPW with the average cost being 1.6 times greater in the ST group (95% CI 1.0733, 2.2887, P = 0.020). While still significantly different, controlling for possible confounding with IPW dropped the cost ratio by approximately 40% (Figure 4).

Hospital costs. Within the whole cohort, the mean cost for same-day (SD) patients was $71,193 compared with $145,907 for staged (ST) patients. For the unadjusted analysis, the average cost was 1.9 times greater in the ST group vs SD group (95% CI 1.6008, 2.2698, P < 0.0001). On IPW, the average cost was 1.6 times greater in the ST group (95% CI 1.0733, 2.2887, P = 0.0203). The mean cost for SD patients with more than 4 levels fused was $93,267.67 compared with $153,481.20 for staged patients. The average cost for the ST group was 1.5 times greater than in the SD group (95% CI 1.2169, 1.8182, P = 0.0002). This significance was again seen using IPW with the average cost being 1.5 times greater in the ST group (95% CI 1.1730, 1.8728, P = 0.0013). Abbreviations: IPW, inverse probability weighting; LS, long segment.
LS Cohort
The mean cost for SD patients with more than 4 levels fused was $93,267.67 compared with $153,481.20 for ST patients. The average cost for the ST group was 1.5 times greater than in the SD group (95% CI 1.2169, 1.8182, P < 0.001). This significance was again seen using IPW, with the average cost being 1.5 times greater in the ST group (95% CI 1.1730, 1.8728, P = 0.001; Figure 4).
Discussion
While our understanding of ASD pathologies and correction techniques has improved exponentially, the complexity of the surgeries combined with the increasing age and age-related comorbidities of the ASD population often complicates the patients’ hospital stays, affects their quality of life, and inflates health care costs.19,20 Proper surgical planning can be critical to mitigating the high morbidity of multiapproach ASD surgeries, including the decision to stage surgeries or combine approaches on the same day.20 The literature, however, still lacks high-quality evidence of the superiority of one strategy over the other.
Three decades ago, Shufflebarger et al retrospectively reported a comparison of ST (n = 35) vs SD (n = 40) corrective surgery for spinal deformity patients. Their data showed significantly shorter operative time and LOS, less blood loss, more favorable deformity correction, and lower postoperative complications rates in the SD group vs the ST group.18 Notably, their patient cohort included several categories of spinal deformity, including congenital and degenerative spinal pathologies, and their protocol for staging the anterior and posterior spinal fusion included 7 to 10 days between procedures. Viviani et al reported a retrospective comparison of 1- (n = 11) vs 2-stage (n = 11) anterior and posterior spinal fusions. The inclusion of patients to either group was based on preoperative risk assessment as well as the feasibility to combine both anterior and posterior approaches that would last for a total maximum operative time of 9 hours. The 1-stage groups showed a significantly more favorable postoperative morbidity profile. Additionally, the 1-stage group showed shorter LOS and less EBL.11
In 2012, Passias et al reported a population-based national discharge data analysis to analyze perioperative outcomes of 11,265 circumferential spine surgeries between 1998 and 2006. They compared SD vs ST circumferential spine surgeries, which showed a higher rate of perioperative complications among the ST group.12 Similar to our findings, the incidence of postoperative venous thrombosis and acute respiratory distress syndrome was significantly higher among the ST group with increasing odds of mortality and morbidity compared with the SD group. In 2017, Passias et al performed another retrospective analysis of prospective multicenter data comparing open ST (n = 71) vs SD (n = 71) spine surgery in ASD patients, utilizing a propensity score matching to adjust for the preoperative differences between both groups. Again, patients in the ST groups had significantly more complications resulting in reoperations. While the incidences of intraoperative complications, infections, wound complications, and 2-year mortality were similar, the incidence of revision surgery at 2-year follow-up remained higher in the ST group.16 Both studies confirm the equal, if not superior, profile of SD compared with ST surgeries.12,16 However, these studies were not limited to circumferential corrective surgeries, which is a unique aspect of our cohort.
There is great variability in the decision-making process that determines whether or not to stage ASD cases among spine surgeons. While surgeons typically utilize the available information about patients’ health to optimize the surgical plan, the differences in surgical training backgrounds and preferences often become important determining factors. Many external factors can also influence the surgical planning of complex spinal deformity correction, including organizational factors such as OR and staff availability, as well as patient preference. Notably, not all health care systems have the same degree of resource availability, which can be a critical factor in planning procedures. This variation also highlights the relative paucity of data comparing ST to SD spinal fusions. Together, this makes it difficult to create generalized guidelines for ASD treatment, which is why we aimed to evaluate outcomes from a large cohort of ASD procedures from a multisurgeon academic center. Studying this patient population in this context limits the variability encountered in different practice settings/institutions. Of note, this patient group consists exclusively of patients who received ALIF and PSF. We deliberately excluded cases that underwent other interbody fusion procedures using any approach that was not an open anterior approach in order to avoid additional variability in the surgical characteristics of both groups and to remove the surgical approach from the potentially confounding factors in our analysis.21
In this present study, we carefully screened the past medical and surgical history of the patient population. Within the full cohort, the ST group underwent significantly more invasive circumferential spine fusions and had more intraoperative and postoperative complications, reoperations, and disposition to inpatient rehabilitation or SNF. As a sensitivity analysis to account for the patient characteristics, comorbidities, and surgical differences between both groups, we utilized IPW to mine for actual significant differences after controlling for possible confounders. Furthermore, in order to appropriately compare SD vs ST procedures and mitigate the differences accounted for by complexity of surgery, the patients were subdivided into those undergoing more than 4 levels of posterior fusion for both unadjusted univariate and IPW analysis. Following these analyses, the differences in perioperative outcomes were no longer significant after IPW except for PE and LOS, which remained significantly higher for the ST group after IPW in both the full cohort and the LS cohort.
Extended hospitalization is independently associated with increased hospital costs after ASD surgeries. This finding has been reported by Stephens et al, who also reported other drivers of increased overall costs such as COPD, diabetes mellitus, number of fused levels, operative time, 90-day readmission, and utilization of inpatient rehabilitation.22 To look further into the implications of the increased LOS, we performed a cost analysis to identify significant differences in hospital costs. This analysis showed significantly higher total hospital admission costs in the ST group, highlighting the expected association between longer hospitalizations and increased costs. Importantly, this finding was seen in the whole cohort and within those patients undergoing more than 4 levels of fusion on IPW. While the extended hospitalizations in the ST group can partially be attributed to the planned staging of the circumferential spinal fusion, it may be attributed to the increased in PE rates in these patients, particularly in those undergoing more than 4 levels of fusion.
Previous reports comparing the 2 strategies often showed worsened morbidity profiles with staging of circumferential corrective surgeries for ASD. One recent retrospective study found postoperative pulmonary complications in 11.7% of adult scoliosis patients with risk factors including a preoperative Cobb angle of >75°.23 A circumferential approach to the spine has been reported to have a higher rate of PE (OR = 1.94) in recent reports.24,25 Our findings further suggest that staging posed an increased risk of PE, led to higher LOS, and ultimately may have increased hospital costs even when accounting for the number of levels fused.
There are several limitations to our study. Given the retrospective, nonrandomized data collection method and analysis, the level of evidence provided from our results is subject to potential confounding and could also lead to selection bias. The decision to undergo ST or SD procedures was made at the discretion of the surgeon. Unfortunately, there was absence of a system to document the reason ASD cases were ST or performed on the SD in each individual case. However, IPW was chosen to mitigate the differences between the groups and create a pseudoexperiment. Additionally, a subgroup analysis was performed of patients undergoing more extensive surgery with a cutoff of more than 4 posterior levels fused. The study also lacks several patient-reported outcomes measures to add further insight into the differences between both surgical strategies. Finally, despite it being one of the largest studies available, the sample size of this study remains relatively low, particularly in those patients undergoing more than 4 levels of fusion. Since many outcomes of interest had relatively low incidence rates, the analysis had limited power, particularly after IPW, and multiple variables showed trending differences but did not reach statistical significance. Therefore, future multi-institutional, prospective randomized controlled trials utilizing greater sample sizes are needed to confirm these findings, make the results more generalizable, elucidate and control for the surgeon’s rationale for selecting ST or SD, and to study the risks of PE in the ST group more closely with documentation of ambulatory schedules, chemical prophylaxis, and sequential compression device usage.
Conclusions
In this study, staging of circumferential ASD corrective surgeries differed from SD surgeries with the rate of PE being significantly higher in patients undergoing ST procedures. This finding was significant regardless of the number of levels fused. Additionally, ST procedures were associated with significantly greater LOS and higher total admission costs.
Acknowledgments
We thank Eileen Maloney-Wilensky and Marie Kerr for providing logistic and administrative support to the research team at the Department of Neurosurgery.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosures The surgeons who performed spine surgery in this cohort included V.A. (65% of the cases), A.K.O. (20%), and W.C.W. (15%).
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}