


Abstract
Background We describe a technique for percutaneous transfacet screw placement in the cervical spine without the need for lateral-view fluoroscopy.
Methods Previously established articular pillar morphometry was used to define the ideal trajectory for transfacet screw placement in the subaxial cervical spine. A unique targeting guide was developed to allow placement of Kirschner wires across the facet joint at 90° without the guidance of lateral-view fluoroscopy. Kirschner wires and cannulated screws were placed percutaneously in 7 cadaveric specimens. Placement of instrumentation was performed entirely under modified anteroposterior-view fluoroscopy. All specimens were assessed for acceptable screw placement by 2 fellowship-trained orthopaedic spine surgeons using computed tomography. Open dissection was used to confirm radiographic interpretation. Acceptable placement was defined as a screw crossing the facet joint, achieving purchase in the inferior and superior articular processes, and not violating critical structures. Malposition was defined as a violation of the transverse foramen, spinal canal, or nerve root or inadequate fixation.
Results A total of 48 screws were placed. Placement of 45 screws was acceptable. The 3 instances of screw malposition included a facet fracture, a facet distraction, and a C6-7 screw contacting the C7 nerve root in a specimen with a small C7 superior articular process.
Conclusions Our data show that with the appropriate radiographic technique and a targeting guide, percutaneous transfacet screws can be safely placed at C3-7 without the need for lateral-view fluoroscopy during the targeting phase. Because of the variable morphometry of the C7 lateral mass, however, care must be taken when placing a transfacet screw at C6-7.
Clinical Relevance This study describes a technique that has the potential to provide a less invasive strategy for posterior instrumentation of the cervical spine. Further investigation is needed before this technique can be applied clinically.
Minimally invasive surgery of the spine is a set of surgical techniques and principles that emphasize soft-tissue preservation while maintaining the established principles of open spinal surgery. Percutaneous pedicle screw placement in the thoracolumbar spine has gained widespread acceptance1–3; however, similar fixation methods have not yet been developed for cervical instrumentation. The advantages of applying minimally invasive surgery principles to the posterior cervical spine include a reduction in muscle damage, decreased blood loss, reduced risk of infection, and the potential for early hospital discharge and return to normal functioning. The risk of infection after open posterior cervical fusion has been reported to be as high as 18%,4 and as with other regions of the spine, this could potentially be dramatically reduced through the use of a percutaneous technique. Potential uses for percutaneous posterior cervical stabilization include supplemental fixation in the setting of multilevel anterior cervical discectomy and fusion or corpectomies; stabilization of pseudarthrosis after anterior cervical discectomy and fusion; and treatment in the setting of trauma, tumor, infection, or deformity surgery for which a circumferential approach is required without the need for posterior laminectomy. Holly and Foley5 described a percutaneous technique for placement of lateral mass screws in the cervical spine relying on isocentric C-arm (Philips Healthcare, Andover, Massachusetts) and image guidance; however, a safe and reproducible technique for percutaneous subaxial cervical fixation with simple uniplanar fluoroscopic guidance has yet to be described.
Many challenges exist with the development of a percutaneous posterior cervical fixation technique, including proximity of critical structures, anatomic variability, radiographic difficulties caused by the overlapping shoulders in the lower cervical spine, and radiation exposure. Transfacet screws may be an ideal option for percutaneous fixation of the postaxial cervical spine. They are simple to place, with no connecting rods, locking caps, or other associated devices. Subaxial cervical transfacet screw placement was first described in 1972, by Roy-Camille and Saillant,6 as an alternative method of fixation when lateral mass screw placement is not available because of fracture. Subsequent cadaveric studies have evaluated the biomechanical properties of transfacet fixation and shown it to be equivalent or superior to lateral mass screw and plate or rod constructs in both pullout7 and flexion, extension, and lateral bending and axial torsion with single-level and multilevel constructs.8, 9
Takayasu et al.10 reviewed the outcomes of 25 patients at 4 months to 5 years in whom a total of 81 subaxial cervical transfacet screws were placed. In 10 instances the transfacet screws were used alone, and in 71 instances they were used as anchors with rods for multilevel fusions. All screws were placed by an open technique with the assistance of lateral-view fluoroscopic guidance. No vertebral artery or nerve root injuries occurred. Five screws appeared loose on subsequent imaging, and all 5 screws had been used in the setting of a rod and screw anchorage for a multilevel construct. One patient required revision. Fusion was achieved in all patients.
Despite evidence to suggest that transfacet screws can be safely applied in an open manner, no feasibility studies have been conducted to assess safe percutaneous placement. In a cadaveric study by Lauren et al.,11 transfacet screws were placed percutaneously using biplanar fluoroscopy in cadaveric specimens. Because of multiple breaches of critical structures, including the central canal and the vertebral artery foramen, the study was discontinued after screw placement in 3 cadavers. The authors concluded that with current instrumentation and techniques, percutaneous placement of transfacet screws cannot be safely performed.
Our study was designed to evaluate the feasibility of a novel technique for percutaneous placement of transfacet screws in the subaxial cervical spine under limited anteroposterior (AP)–view radiographic guidance in a cadaveric model using a unique radiographic targeting device and radiographic technique. In addition, we describe a novel radiographic view designed to facilitate the technique. Our goal was to evaluate the accuracy of screw placement; the risk to surrounding vital structures, including the central canal, exiting nerve roots, and vertebral artery; and the success of immobilization of the facet joint.
Methods
Specimen preparation
Ten fresh-frozen cadaveric cervical spines from C1 to C7 were harvested and stripped of skin and subcutaneous fat. Paraspinal musculature was left in place. The specimens were evaluated radiographically to rule out previous surgery, deformity, and advanced spondylosis that would make obtaining appropriate fluoroscopic views impossible. Before use, each specimen was thawed to room temperature. The specimens were mounted on a custom jig (Fig. 1) that allowed for manipulation of flexion, extension, and rotation and were placed on a radiolucent table.

Specimen mounted for instrumentation.
Percutaneous screw placement technique
Screw placement was accomplished bilaterally at the C3-4, C4-5, C5-6, and C6-7 levels under modified AP-view fluoroscopic guidance only (the “facet AP view”), with no lateral-view fluoroscopy. Previously described articular pillar morphometry12–15 was used to define a start point in the upper third of the lateral mass at a point 1 mm medial to the midline of the cranial facet (1 level higher than the instrumented level). A medial-to-lateral trajectory of approximately 20° was used, aiming for a point 1 mm lateral to the midline of the facet joint to be instrumented. A cranial-tocaudal trajectory that was perpendicular to the instrumented facet joint was used. With the guide in proper position, a guidewire was placed across the facet joint. A cannulated drill was then used over the guidewire to create a bone hole, and a cannulated screw was next inserted. A screw length of 14 mm was selected in each case. No lateral-view fluoroscopy was used during the instrumentation procedures.
Novel radiographic technique
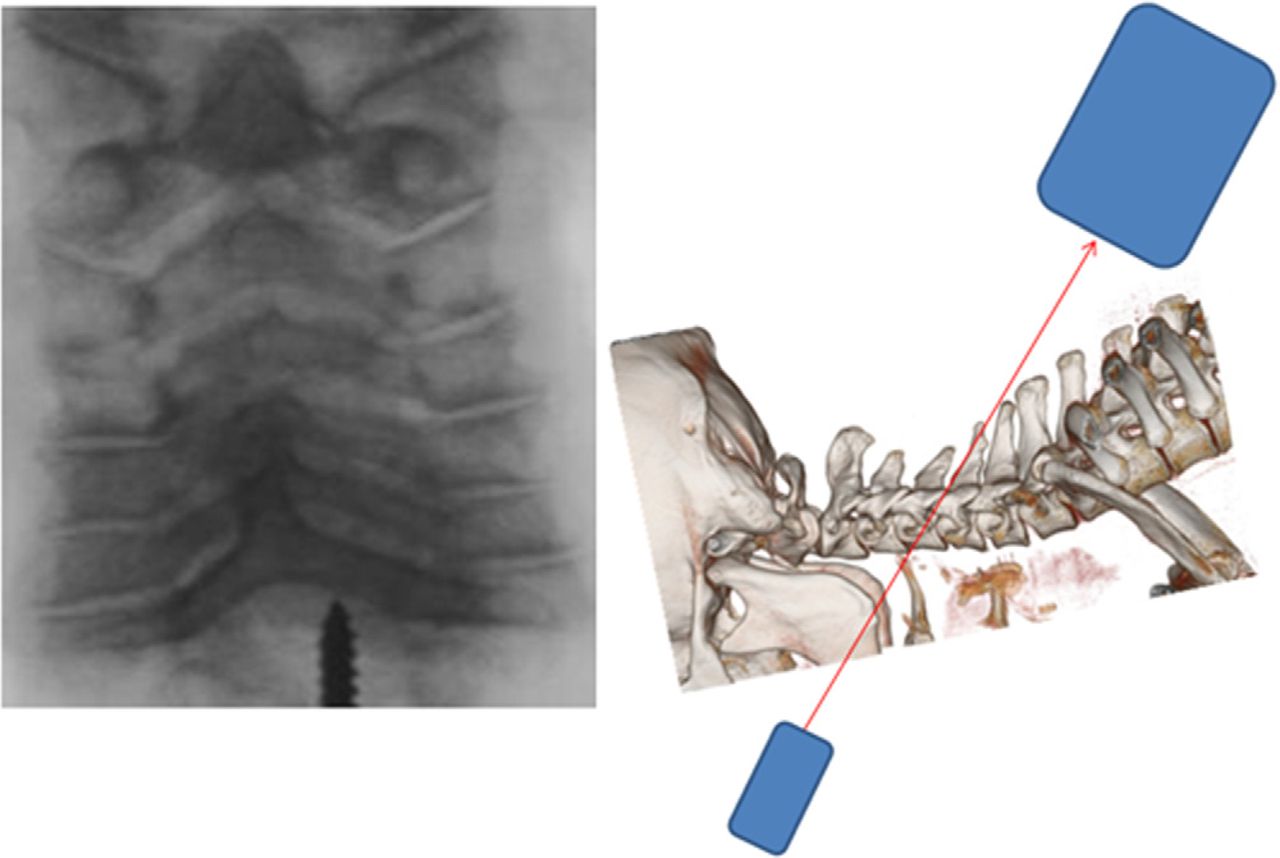
The facet AP view is a modification of the standard cervical AP view with the C-arm beam angled parallel to the facet joint being instrumented (Figs. 2 and 3). The facet AP view directly determines the starting point and the mediallateral trajectory of the screw but not the cranial-caudal trajectory. A radiographic targeting guide was designed that would indirectly ensure a cranial-caudal trajectory perpendicular to the facet joints under the facet AP view. Accurate positioning for this view is critical, and the exact position may be different for each facet level.

Standard AP view. The beam is angled parallel to the disc spaces, providing an oblique view of the joints.

Facet AP view. The patient is placed in the Trendelenburg position, and the C-arm is angled such that the beam is parallel to the facet joint being instrumented (in this case, C4-5). The joint appears as a clear space on the monitor.
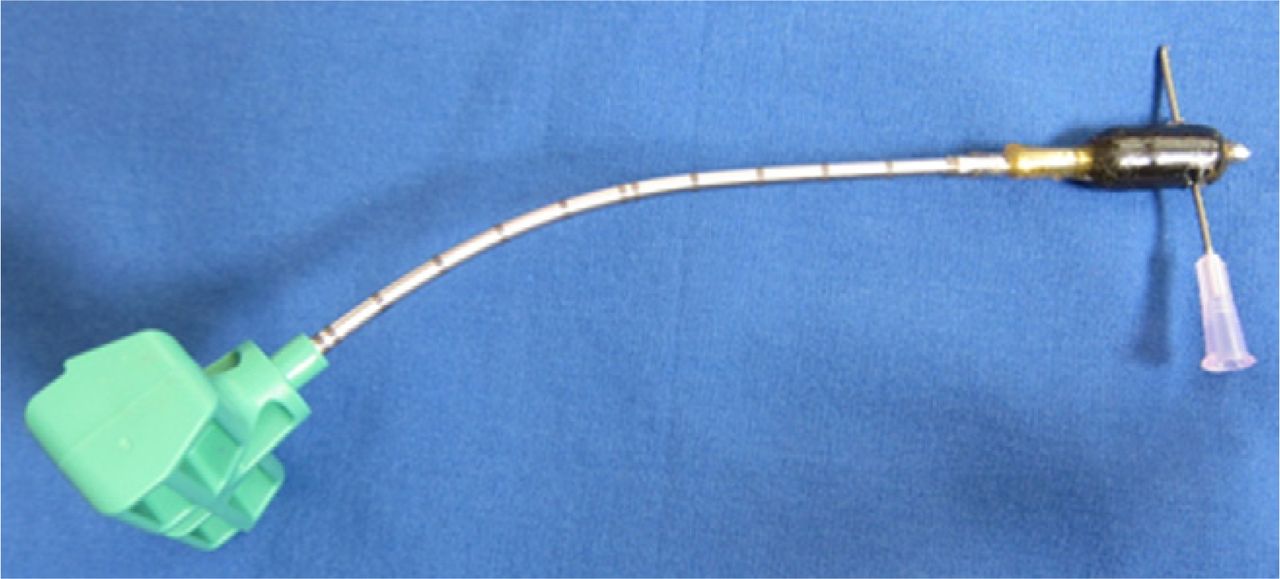
The radiographic targeting guide relies on Euclid's fifth postulate (the parallel postulate), which states that a straight line crossing 2 parallel planes crosses each plane at complementary angles. Therefore, if the C-arm beam is parallel to the facet joint, a straight line crossing at 90° to the C-arm beam will also cross at 90° to the facet joint. To implement this concept, a radiographic targeting device was designed to accurately indicate when the drill is perpendicular to the C-arm beam and therefore perpendicular to the facet joint. The guide comprises a radiopaque cannula with a small radiolucent hole perpendicular to its longitudinal axis. The cannula is placed on the lateral mass at the starting point and is angled until the hole becomes visible on the fluoroscopic image. At that point, the hole is parallel to the C-arm beam, and the cannula is perpendicular to the C-arm beam and to the facet joint (Fig. 4). We fabricated our targeting device (Fig. 5) from a bone marrow aspiration trocar (chronOS; Synthes Spine, Monument, Colorado) made radiopaque with leaded fabric from a thyroid protection shield (Burlington Medical Supplies, Newport News, Virginia) and sealed with epoxy. The guide was bent to allow for easier placement, and the targeting hole was made with an 18-gauge needle.

Guide placed perpendicular to C-arm beam, confirmed by targeting hole.

Radiographic targeting device. The 18-gauge needle passing through the radiopaque section perpendicular to the longitudinal access should be noted. Under the facet AP view, when this hole is visible on the fluoroscopic image, the guide will be perpendicular to the beam and therefore perpendicular to the facet joint.
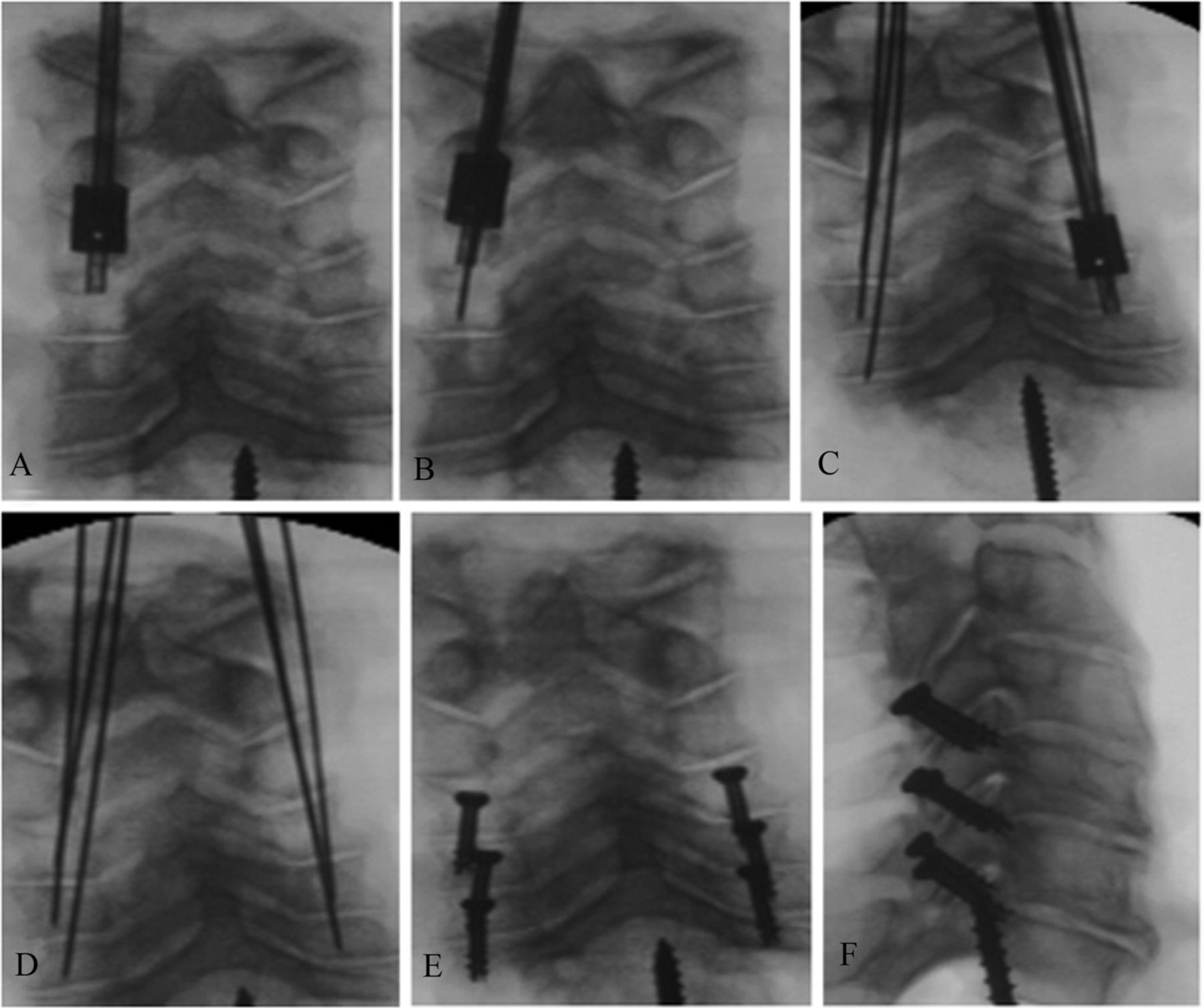
To place the transfacet screws, a perfect facet AP view was first obtained. Care was taken to ensure proper rotation of the segment by verifying that the spinous process was midline at each level. Next, a No. 15 blade was used to split the paraspinal tissues, and the targeting guide was placed at the starting point in the upper third of the lateral mass, 1 mm medial to the midline of the facet above, angled laterally toward a point 1 mm lateral to the midline of the facet joint to be instrumented. Cranial-caudal angulation was adjusted until the targeting hole came into view. A Kirschner wire (K-wire) was placed down the guide and advanced to the level of the joint. This was repeated for all levels instrumented, with the C-arm being adjusted at each level to ensure a perfect facet AP view. After all K-wires were placed, self-drilling or self-tapping 14 × 4–mm cannulated screws were placed over the wires and the wires were removed (Fig. 6). All instrumentation was performed by an orthopaedic spine surgery fellow under the guidance of fellowship-trained orthopaedic spine surgeons.

Screw placement technique. (A) The guide was placed at the starting point, and cranial-caudal angulation was adjusted until the targeting hole came into view. (B) A K-wire was placed down the guide and advanced to the level of the joint. (C) This was repeated for all levels instrumented, with the C-arm being adjusted at each level to ensure an accurate facet AP view. (D) All K-wires were placed. (E) Self-drilling or self-tapping 14 × 4–mm cannulated screws were placed over the wires, and the wires were removed. (F) The lateral view confirms screw placement.
Evaluation of screw placement
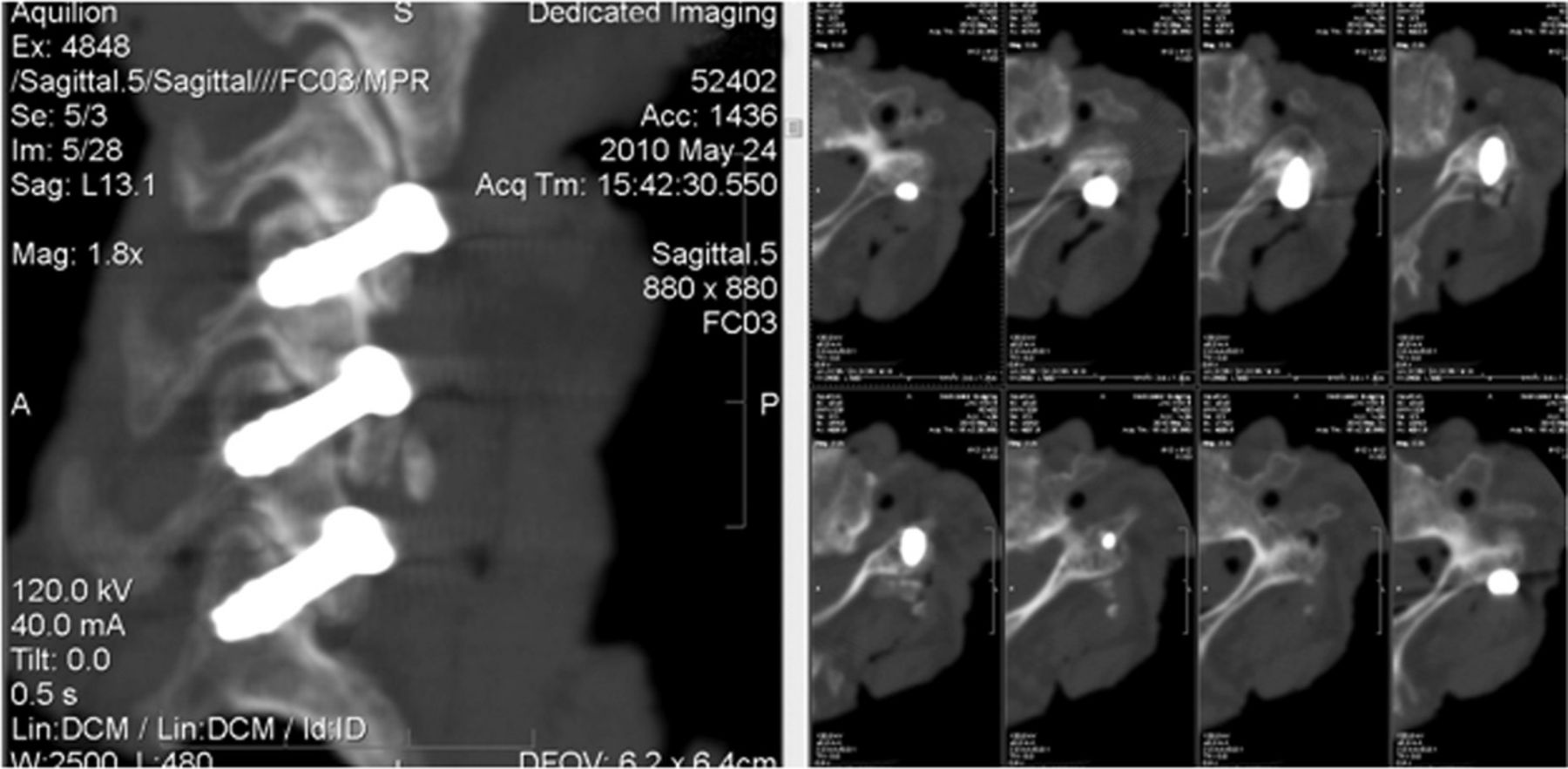
Screw placement was evaluated with the use of computed tomography (CT) (Fig. 7) and by direct visualization (Fig. 8). Acceptable screw placement was defined as a screw that achieved purchase in the inferior and superior articular processes, crossed the facet joint, and did not violate the central canal, nerve roots, or vertebral artery. Breach was defined as any screw that violated a critical structure or failed to achieve purchase across the joint. After instrumentation, all specimens were evaluated for screw placement with the use of CT reviewed by 2 fellowship-trained spine surgeons and for nerve root injury by direct dissection.

Acceptable screw placement confirmed by CT.

Direct nerve root dissection.
Results
Of the 10 cadaveric specimens obtained, 7 were used for this study; 3 specimens were found to be unsuitable because of advanced spondylosis that precluded accurate imaging. We instrumented 24 of 28 potential levels, for a total of 48 screws placed. Screws could be placed bilaterally in all specimens at the C4-5 and C5-6 levels; however, 4 screws at C3-4 and 4 screws at C6-7 could not be placed because of the inability to obtain optimal facet AP views. Of the 48 screws inserted, 45 were deemed to be in acceptable position. Three breaches occurred (Table 1). The first breach was a facet fracture at the C5-6 level. The screw was placed slightly low and was overtightened, resulting in fracture of the C5 inferior articular process and over-advancement of the screw (Fig. 9). The second breach was distraction (rather than fixation) at the C3-4 level. This occurred because a screw failed to achieve purchase in the superior articular process at C4 and therefore distracted the facet (Fig. 9). The final breach was a screw that violated the neural foramen at C6-7 (Fig. 10).

Breaches. (A) Facet fracture (bottom screw). (B) Distraction.

C6-7 nerve root injury. In a specimen with a small C7 superior articular process, the screw is seen passing through the bone and into the neural foramen. Direct dissection shows that the screw is in the neural foramen, displacing the C7 nerve root superiorly and anteriorly.
Results
Discussion
We describe a new technique for percutaneous transarticular screw placement in the subaxial cervical spine that uses a unique radiographic targeting guide to allow the surgeon to attain the proper screw trajectory while relying on only a specialized radiographic view (the facet AP view). We were able to successfully instrument a series of cadaveric specimens using this technique.
An analysis of the breaches is helpful in discussing the safety of this technique. The first breach, a facet fracture, occurred because the screw was placed low and was overtightened. Our guide rendered reproduction of an accurate starting point difficult because its inner diameter was significantly larger than the K-wire being placed. This disparity allowed for some variation in the K-wire entry site. Furthermore, the acute angle between the guide and the posterior cortex of the lateral mass resulted in a tendency toward creating a more distal starting point. A more refined guide may avoid this problem.
The second breach resulted in a distracted facet. This may have been avoided had we penetrated deeply enough with the drill before placing the self-tapping screw.
One screw caused nerve root impingement even though it was placed with proper technique. This breach occurred at C6-7. The facet joint appeared to be properly instrumented; however, we found a violation of the neural foramen with displacement of the nerve root caused by screw contact. The C6-7 level presents a unique problem with this technique because of the variability of the C7 anatomy. The C7 lateral mass represents a transitional level between cervical and thoracic. Often, the superior articular process at C7 is thin and elongated, resulting in a more vertically oriented joint.13, 16, 17 Although we found that a thin superior articular process may not be suitable for transfacet screw placement, other C7 superior articular processes are more robust and can safely accept a transfacet screw (Fig. 11). In our study we were unable to instrument 4 of the 14 C6-7 levels because we were unable to obtain a clear facet AP view.

Variable C7 superior articular facet anatomy, as noted in our study. (A) A thin, vertical C7 superior articular process that is not appropriate for screw placement. (B) A C7 superior articular process that is ideal for screw placement.
This is likely partly because of the variable anatomy at this joint. However, simply being able to obtain a facet AP view of the C6-7 joint does not eliminate the risk of nerve root injury. On the basis of this experience, one might consider advanced imaging (such as CT) to evaluate the size of the C7 superior articular facet before attempting transfacet screw placement at C6-7.
This work represents a preliminary cadaveric study of a novel technique for transfacet screw placement in the cervical spine. It presents a new type of radiographic navigation that may be a viable way to indirectly determine screw trajectory in multiple planes without the need for biplanar fluoroscopy. The drawbacks of this study lie in the rudimentary nature of its design. The specimens were not intact cadavers but were cadaveric cervical spines with the muscle left in place. Removing the head and torso from the field made mounting the specimens and obtaining the facet AP view much easier; however, in practice, the head, jaw, and torso may impact one's ability to obtain a facet AP view of each level. The goal of our study design was to eliminate as many confounding variables as possible to learn whether our technique was viable and thereby warranted further study. We elected to disarticulate the cervical spines and remove the skin because this allowed for a more consistent environment. Initial testing was conducted with intact torsos, and during that initial testing, we found that the teeth posed the greatest problem. In specimens without teeth, visualization was easy because the mandible is thin and relatively radiolucent compared with the lateral pillars. However, in specimens with teeth in place, especially those with dental implants, the teeth posed a considerable obstacle to visualization of the upper levels. Further study is required to determine whether this radiographic technique can be applied to all cervical levels clinically.
Another drawback of this study was that it failed to assess the safety of all aspects of our technique. Although we evaluated the specimens for violation of critical structures after final instrumentation, we did not assess for such violation during K-wire placement or drilling. Considering that the study was conducted during the most preliminary testing portion of technique development, our instrumentation was rudimentary and might not reflect the final surgical technique. Before clinical application, our instrumentation and technique must be refined and all steps of the procedure, including wire placement and drilling, must be tested and shown to be safe.
Conclusion
Transfacet screws may represent an improved type of percutaneous fixation technique in the subaxial cervical spine when posterior fusion or open decompression is not required. We describe a novel technique for screw placement that uses a unique radiographic targeting device to allow for multiplanar targeting under a single fluoroscopic view. By using this technique, we were able to successfully instrument cadaveric cervical spines. Further study is needed before this technique can be applied clinically. However, this technique has the potential to provide a novel, less invasive strategy for posterior column instrumentation in the cervical spine while minimizing operative time and radiographic exposure for the patient, surgeon, and operating room staff. Although this study is rudimentary and does not conclude that this technique is safe or applicable clinically, it introduces a new novel technique of radiographic targeting that, pending further study, might one day be the basis for useful clinical intervention in the context of cervical facet screw placement or other applications.
Acknowledgments
The authors thank senior editor and writer Dori Kelly, MA, University of Maryland School of Medicine, for assistance with the manuscript and the figures.
Footnotes
This study was funded by an unrestricted educational grant from Synthes Spine. No benefits in any form have been received from a commercial party related directly or indirectly to the subject of this manuscript.
- © 2012 Published by Elsevier Inc. on behalf of ISASS - International Society for the Advancement of Spine Surgery.
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.