


Abstract
Sacropelvic (SP) fixation is the immobilization of the sacroiliac joint to attain lumbosacral fusion and prevent distal spinal junctional failure. SP fixation is indicated in numerous spinal conditions (eg, scoliosis, multilevel spondylolisthesis, spinal/sacral trauma, tumors, or infections). Many SP fixation techniques have been described in the literature. Currently, the most used surgical techniques for SP fixation are direct iliac screws and sacral-2-alar-iliac screws. There is currently no consensus in the literature on which technique carries more favorable clinical outcomes. In this review, we aim to assess the available data on each technique and discuss their respective advantages and disadvantages. We will also present our experience with a modification of direct iliac screws using a subcrestal approach and outline the future prospects of SP fixation.
INTRODUCTION
Sacropelvic (SP) fixation is the surgical immobilization of the sacroiliac joint with the aim of preventing distal spinal junctional failure by taking stress off the sacral screws.1 The SP junction is a biomechanically complex region owing to the complex regional anatomy and the high mechanical stress. Moreover, numerous factors may play a role in the technical challenge and the clinical outcomes of SP fixation (eg, poor bony quality and the complex anatomical landscape of the region).1,2 SP fixation is a widely used surgical procedure that is indicated for numerous conditions, such as scoliosis; spinal/sacral trauma, tumors, or infections; as well as multilevel spinal fusions, especially fusions spanning more than 5 vertebral levels incorporating S1, which necessitate additional instruments to reduce the stress on the S1 screw and promote arthrodesis.2,3 Other indications may include the presence of advanced osteoporosis, sacral fractures, correction of lumbar spine deformity, and pelvic obliquity abnormalities in children with neuromuscular deformities (eg, cerebral palsy).1,4
Over the years, many SP fixation techniques have been described in the literature, including Jackson intrasacral rods, Galveston iliac rods, Kostuik transiliac bar, iliosacral screws, sacroiliac buttress screws, iliac screws, and sacral-2-alar-iliac (S2AI) screws.1,5–8 Currently, the most common techniques for SP fixation are the direct iliac screws and S2AI screws, both of which achieve the highest rates of SP fixation and represent biomechanically superior surgical modalities when compared with the former techniques.3,9,10 Since the introduction of these 2 techniques, continuous refinement has been implemented to maximize favorable outcomes (eg, modified subcrestal insertion technique of conventional iliac screws, robotic and freehand-assisted S2AI screws insertion, and augmented reality-navigated screw insertion).11–13
While the current literature outlines the benefits of the direct iliac screws and S2AI screws, the current data available are lacking solid evidence as to which technique is clinically superior.12,14,15 In this review, we aimed to assess the current literature to provide the reader with comprehensive evidence for each technique and respective clinical outcomes for patients requiring SP fixation. Additionally, we describe our institutional experience of subcrestal iliac screw placement, highlighting the nuances of this technique.
ILIAC SCREWS APPROACH FOR PELVIC FIXATION
Conventional Iliac Screws Technique
Iliac screws are one of the most used techniques for SP fixation.2,3,5 Iliac screws are anchors that are placed into the iliac bone bilaterally and connected to the sacrum with rods.16 These screws often require the placement of offset connectors to the native rod.17,18 The iliac screw diameters range from 7 to 10 mm and 100 mm in length for adults, on average.19 Unfortunately, due to the fact that the screw head is relatively superficial, there is a high rate of discomfort, occasional wound dehiscence, and infection.20 Additionally, in some reports, iliac screws were associated with high rates of instrumentation failure.21
The placement of iliac screws often requires extensive dividing and devascularizing of the iliac muscle. The trajectory for placement begins at the posterior superior iliac spine (PSIS) toward the acetabulum and ends at the anterior superior iliac spine (Figure 1).22 Iliac screws are associated with a relatively higher rate of successful SP fusion compared with former commonly used techniques.23,24 Additionally, direct iliac screws often require the placement of bulky offset connectors, adding more stress force on the rod, requiring more operative time, creating a logistic burden, and increasing the risk of postoperative instrumentation prominence.14,25,26

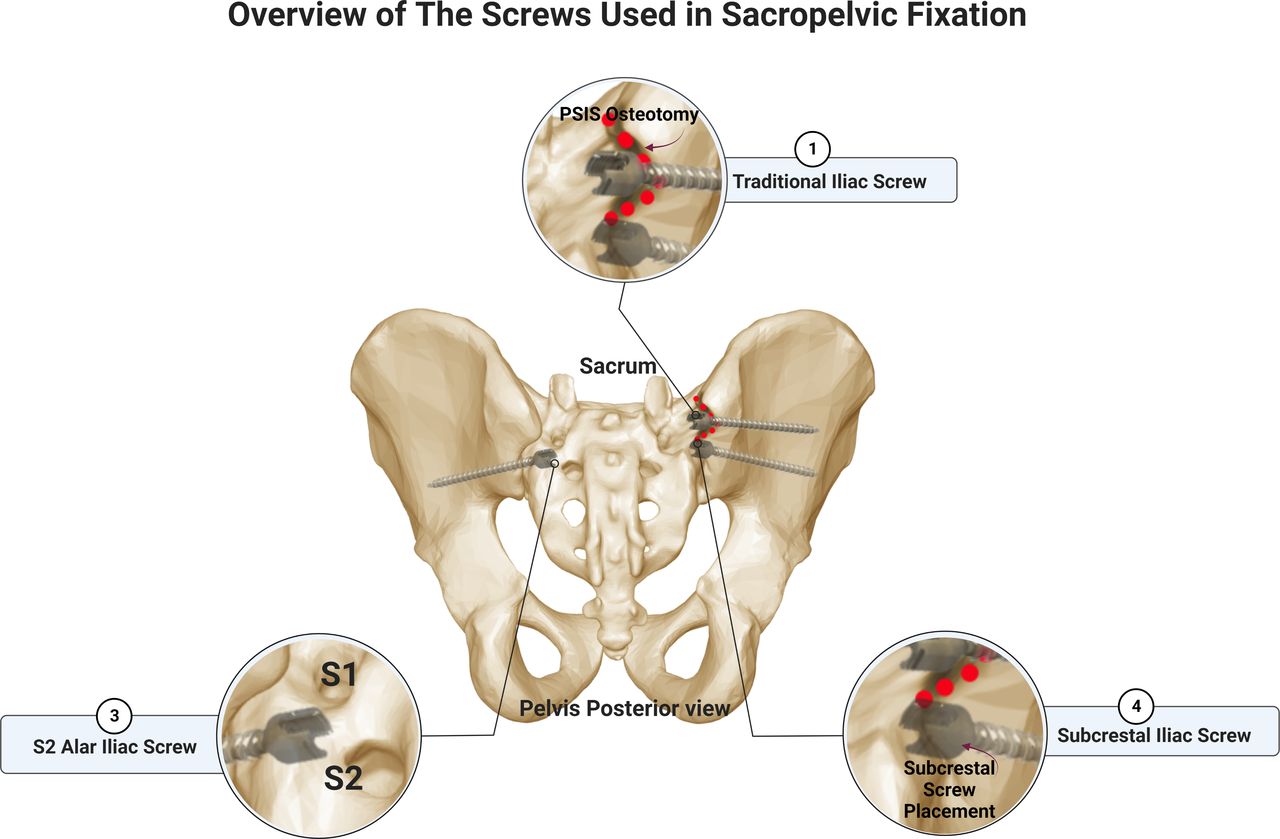
A graphical representation summarizing screws used in pelvic fixation. PSIS, posterior superior iliac spine; S1, sacral 1; S2, sacral 2.
Although most of the literature available describes direct iliac screw utilization as a technique with relatively higher rates of postoperative complications when compared with S2AI screws, some studies have shown lower rates of complications associated with this technique. Nguyen et al27 analyzed the outcomes in 260 adult patients who underwent fluoroscopic-assisted posterior approach iliac screws placement with a 2-year minimum follow-up. The authors stated that the iliac screw heads were placed deeply into the PSIS. Twenty patients (7.7%) had iliac screw-related complications that included screw loosening (9 patients, 3.5%), rod or connector fracture below S1 (11 patients, 4.2%), L5-S1 pseudarthrosis (23 patients, 8.8%), and S1 screw fracture (4 patients, 1.5%). The rate of reoperation was 17.7%. None of the patients in their study reported screw head prominence, required revision surgery, experienced pain, wound dehiscence, or poor cosmesis. The authors concluded that iliac screw fixation techniques should remain a gold standard technique for SP fixation.
Modified Subcrestal Iliac Screws Technique
Anatomically, the entry point for the conventional iliac screw placement is the PSIS, which is very close to the outer skin and, in turn, leads to potential screw head prominence-related complications.20 In the subcrestal iliac screw technique, the entry point is on the medial side of the iliac crest, where the screw is inserted beneath the iliac crest avoiding the sacroiliac joint. This technique allows for low-profile screw insertion and reduces screw head prominence (Figure 1).12
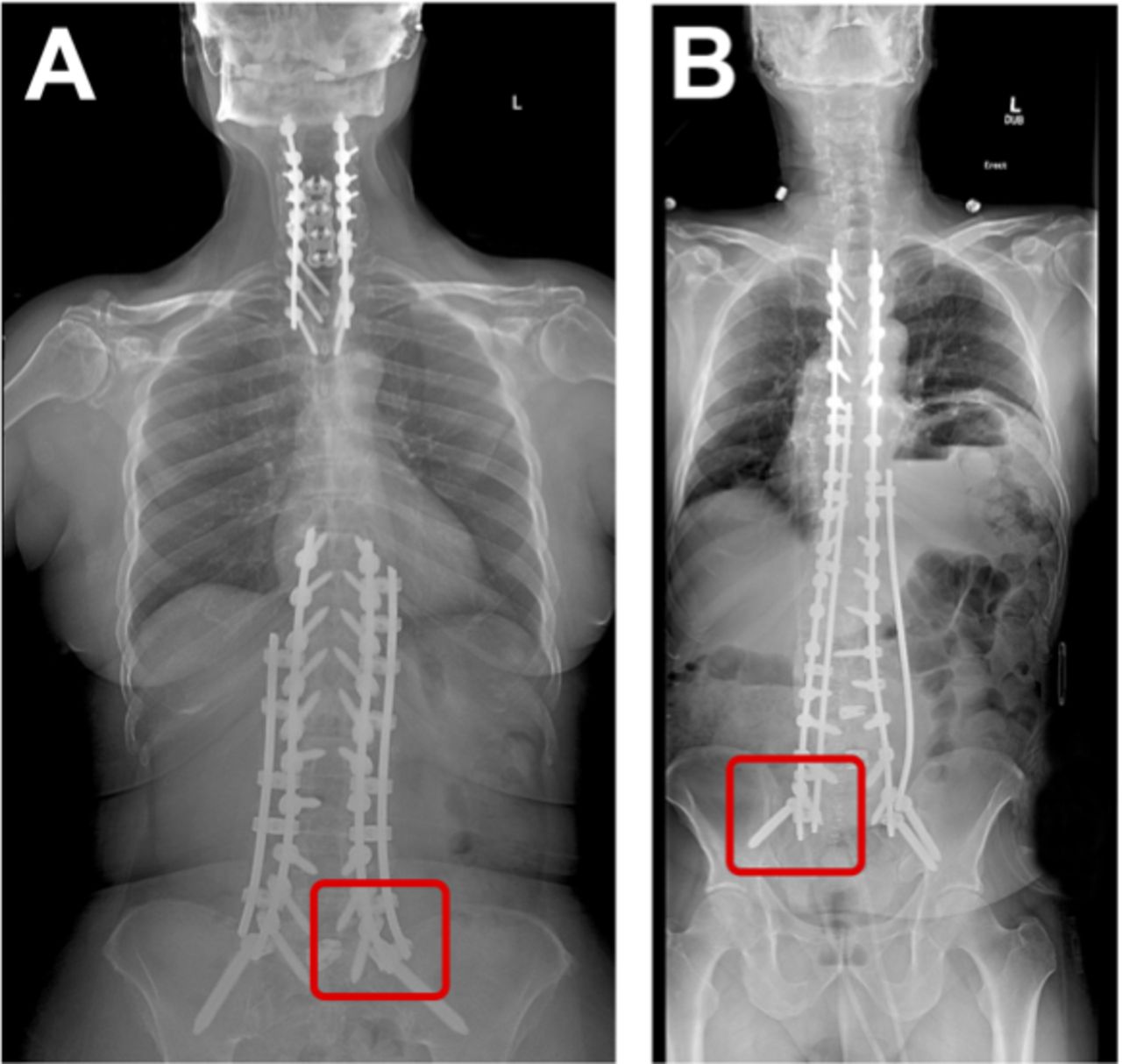
In our experience, we place the subcrestal screw, with 1 screw head inferior and 1 screw head lateral to the S1 pedicle screw on the medial surface of the iliac crest. This allows for a low-profile screw, and with the favorable angle of the screw heads, the rod connects seamlessly with rostral instrumentation resembling the Eiffel tower silhouette (Figures 2 and 3). This method takes into consideration the appropriate lateromedial trajectory of an S1 screw and spares the surgeon any unnecessary dissection of the gluteal muscles, which may result eventually in extensive local muscular degeneration as the screw entry point is on the medial surface (Figure 4). In addition, by placing a slightly longer native rod at the distal junction, one can place a side connector below the subcrestal iliac screw to attach an accessory rod to span the entire construct medially (Figure 2). This allows shielding of the stress between S1 and the iliac screw and provides more stiffness and structural support to promote arthrodesis.

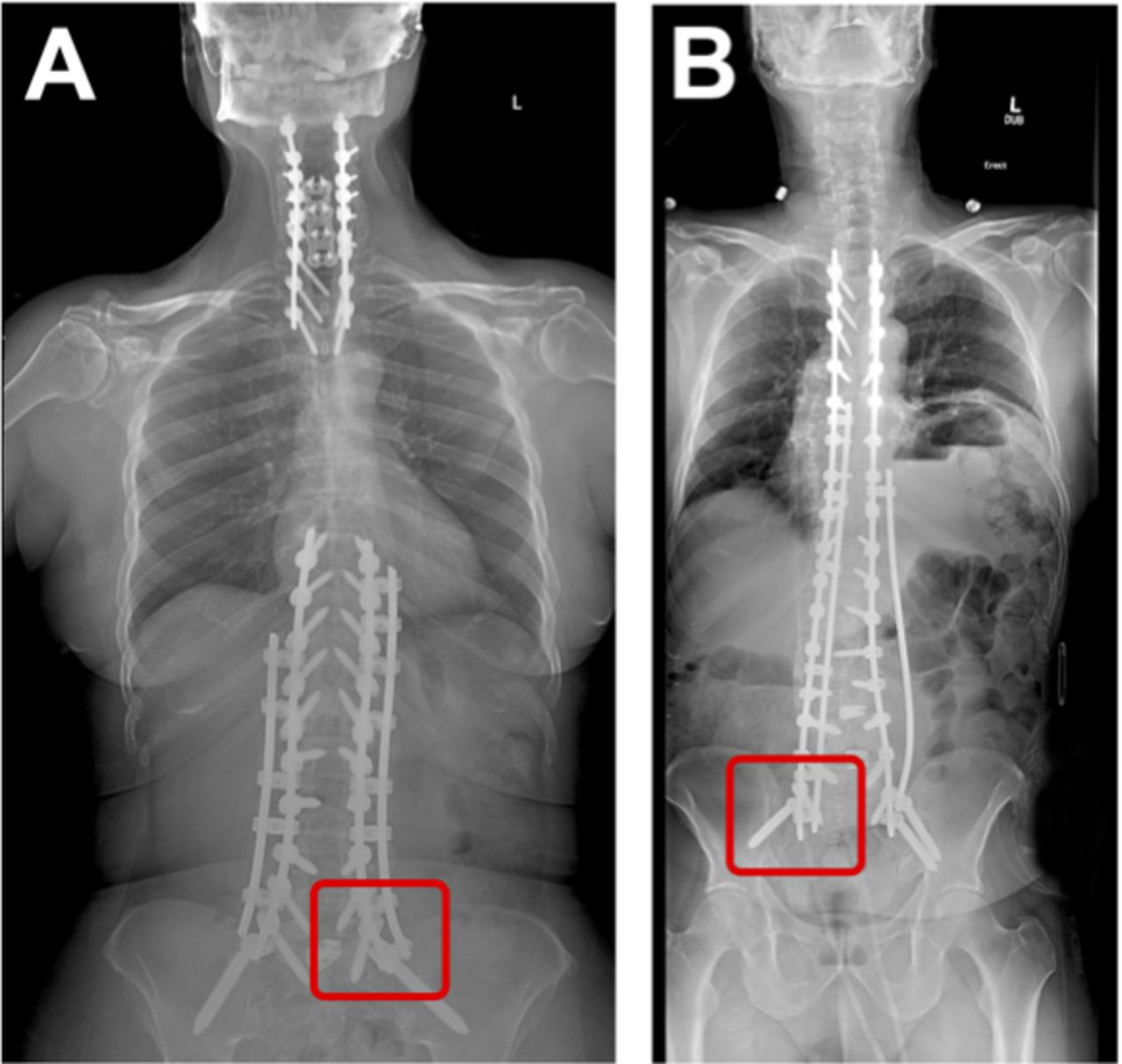
Panels A and B: Postoperative anterior-posterior and lateral x-ray image showing the continuity of the subcrestal fixation construct “Eiffel Tower-like.”
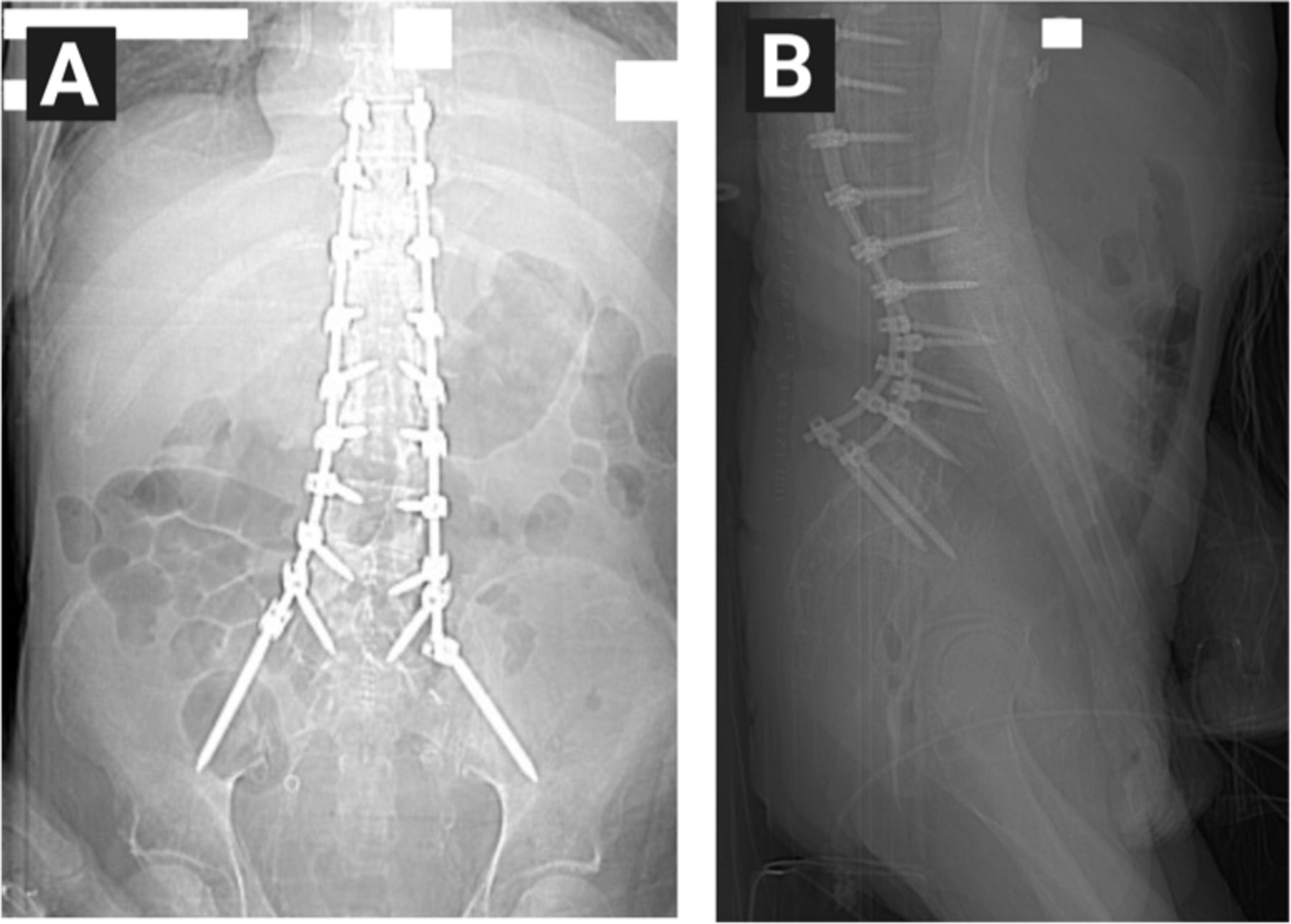
Panels A and B: Postoperative anterior-posterior x-ray image showing the accessory rod connected below the iliac bolt to relieve the stress between S1 and the iliac screw (red square).
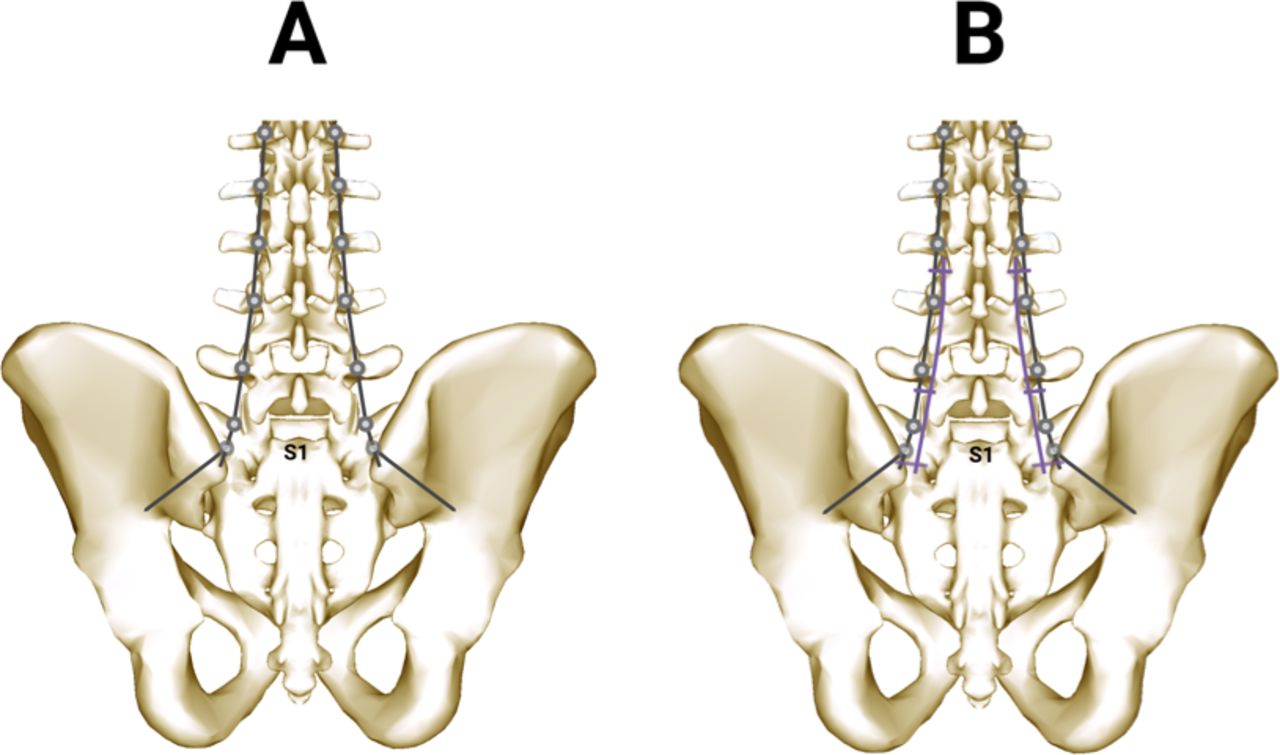
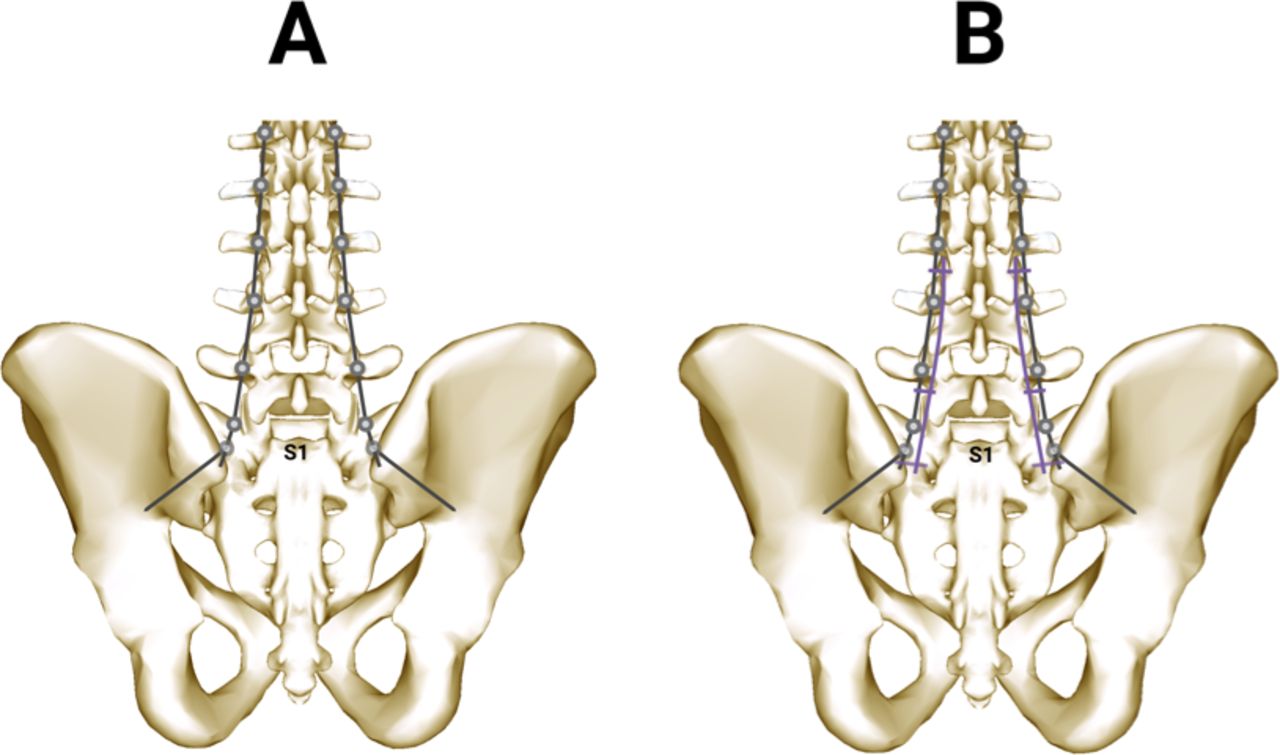
A graphical representation depicting the location for subcrestal screws placement and the accompanying rod spatial orientation.
While the available data regarding subcrestal iliac screws are scarce, the current evidence shows that subcrestal iliac screw insertion is feasible, safe, and results in a significant reduction of iliac screw head prominence and prominence-related complications.12,15 Additionally, subcrestal iliac screws eliminate the use of offset connectors, significantly reducing the rod construct complexity and, in turn, the overall cost. Liu et al investigated the outcomes of subcrestal iliac screw insertion in 10 patients with spinal deformities over a 29-month follow-up period.12 At the last follow-up timepoint, only 1 subcrestal iliac screw head was prominent, and the patient experienced no associated pain. None of the study participants required reoperation, experienced postoperative pain, or had instrument failure. In another study, the same group of authors demonstrated the effectiveness of minimally invasive dual subcrestal iliac screws insertion in the setting of metastatic lumbosacral fracture.15 Von Glinski et al reported improved clinical and radiological outcomes following the use of a similar technique of subcrestal insertion of iliac screws in patients undergoing lumbopelvic fixation.14 In their study, the authors retrospectively compared the clinical outcomes between the conventional iliac screw (n = 40), modified subcrestal screw group (n = 113), and S2AI (n = 37) screw, finding no statistically significant differences between the 3 groups in terms of complications. Additionally, patients in the subcrestal screw group did not report any prominent instrumentation besides experiencing the lowest rate of instrumentation failure across all groups.
Recently, a study by Luo et al showed that the use of subcrestal iliac screw fixation is associated with greater correction of lumbar lordosis and a possible increase in pelvic incidence when compared with S2AI screw in patients treated for adult spinal deformity.28 They described the iliac screw entry point as approximately 10 mm between the posterior edge of the iliac crest and the posterior surface of the sacrum and connected with a lateral connector to the rod below the S1 pedicle screw. Additionally, the screw was deeply inserted, making the screw head flush with the cortex of the iliac bone with the aim of lowering the risk of screw prominence. This study, along with the previously mentioned studies, points out that subcrestal iliac screws combine the benefit of higher fusion rates, the lower incidence of instrument prominence, and the correction of lumbar lordosis.
S2AI SCREW TECHNIQUE FOR SACROPELVIC FIXATION
The S2AI screw technique was described in 2007 by Kebaish et al.29 S2AI screws offer a novel alternative to the conventional iliac screws technique.30 Anatomically, the S2AI screw placement begins at the sacral ala, midway between the S1 and S2 dorsal sacral foramina (Figure 1).31 S2AI screws are placed 15 mm deeper than iliac screws.25,32 This translates into significantly lower rates of screw prominence-related complications.20,33 Additionally, the S2AI screw is aligned in line with the S1 screws, eliminating the need for an extended lateral dissection. Moreover, the S2AI screws fall in line with the cephalad construct, which makes rod insertion easier with no need for rod connectors.26,34 While the S2AI screw technique is mainly reported in spine-related conditions, some studies have demonstrated the use of this technique to treat posterior pelvic ring injuries that resulted in a limited lumbosacral range of movement.35,36
Generally, fixation screws are placed under the guidance of fluoroscopy.37 Nevertheless, the S2AI screws can also be inserted using other methods, such as stereotactic navigation or under the guidance of robotics.38 Another method of inserting S2AI is the freehand method, which relies heavily on the sacropelvic region anatomic landmarks and enables the surgeon to avoid using the traditional fluoroscopy. This method has shown to be a safe and reliable method for SP fixation.39,40
The goal of S2AI SP fixation technique is to achieve a biomechanically stable fixation construct. On testing the biomechanical attributes of the S2AI fixation, the results showed a nonsignificantly increased S2AI fixation construct sturdiness compared with the traditional iliac screws technique.41 The studies available discussing the biomechanical attributes of the S2AI screws and the direct iliac screws are scarce. Further investigational studies are encouraged. Finally, the S2AI screw insertion technique is generally safe in both adults and pediatric patients and is associated with relatively low rates of pseudarthrosis and lower rates of complications.34
DISCUSSION
A plethora of comparative studies are available that compared the efficacy and clinical outcomes of the direct iliac screw and the S2AI screw. In the meta-analysis by De la Garza Ramos et al,42 they analyzed multiple studies with a pool of 323 adult patients (147 in the iliac screws group [45.5%] and 176 in the S2AI group [54.5%]). They found that reoperation due to instrument failure or wound-related complications was required in 66 patients. The overall rate of reoperation was rate 20.4% (27.9% in the iliac screws group vs 14.2% in the S2AI group, P < 0.001). Four studies in the pooled analysis reported wound infections with an infection rate of 12.6% in the S2AI group vs 25.4% in the other group (P < 0.001). Additionally, 3 studies reported screw prominence pain (9.8% in the S2AI group vs 18.1% in the other group, P < 0.001). Similarly, Ha et al investigated the role of S2AI fixation in adult spinal deformity in a 2-year follow-up study with a study population of 83 patients.43 They found that the S2AI screw-related pain rate was 9.6%. An S2AI screw complication was identified in 10.8% of the patients. Such rates are significantly lower than those reported for iliac screw patients in most of the literature.
The outcomes of both techniques were reported in the pediatric population. Tavares-Júnior et al performed a comparative computed tomographic study comparing the iliac screws with the S2AI screws in children.44 They found that the S2AI screw trajectory was associated with greater bone thickness and screw-to-skin distance compared with the iliac screws group. Additionally, Lee et al compared the S2AI screws and iliac screws technique used in pelvic fixation for neuromuscular deformity in pediatrics.45 They found that in a group of 50 patients (22 patients with S2AI screws and 28 patients with iliac screws) with a follow-up of 3.5 ± 1.7 years, the rate of radiographic instrument failure was significantly lower in the S2AI group (57% vs 27%, P = 0.02). They reported no difference between the 2 groups regarding postoperative complications.
The effectiveness of these techniques was assessed in the geriatric population as well. Ishida et al46 compared the safety profile of SP fixation in geriatric patients above 60 years of age between S2AI screws and conventional iliac screws. They analyzed a total of 60 patients (43 patients with S2AI screws and 17 patients with conventional iliac screws) and found that the S2AI screws group experienced lower rates of reoperation (18.6% vs 47.4%; P = 0.02), wound infection (2.3% vs 29.4%; P = 0.006), wound dehiscence (2.3% vs 29.4%; P = 0.006), and lower volume of blood loss (1846.4 vs 2721.2 mL; P = 0.02). Additionally, the rates of L5-S1 pseudarthrosis were similar in both groups. The authors concluded that the use of S2AI in geriatric patients was superior to the use of conventional iliac screws. Another study from the same group was dedicated to radiographically investigating the symptomatic screw prominence in patients with S2AI screws and conventional iliac screws.20 The mean follow-up period in that study was 22.0 months, with 100 total patients (68 patients with 148 S2AI screws and 32 patients with 72 iliac screws). The authors found that there was significantly more symptomatic screw prominence in the iliac screw group (11.1% vs 1.4%, P = 0.002). Additionally, the distance from screw head to skin ≤23 mm was the strongest predictor of symptomatic pelvic screw prominence, with a sensitivity of 100% and specificity of 94.1%. The authors concluded that the use of S2AI screws was associated with a reduced rate of symptomatic screw prominence. Moreover, the distance from screw head to skin ≤23 mm was the strongest predictor of symptomatic screw prominence.
Postoperative complications were compared in numerous other studies. Gao et al in their analysis of 365 patients found that 22% of the patients who underwent iliac screws SP fixation experienced surgical site infection vs 8% in S2AI screws patients.10 Other iliac screws-related complications reported by the same group were: reoperation (28% vs 13% in the S2AI group), screw loosening (20% vs 8% in the S2AI group); screw breakage (12% vs 2% in the S2AI group), implant prominence (14% vs 2% in the S2AI group), pseudarthrosis (15% vs 3% in the S2AI group), and less blood loss (2708.4 vs 2035.4 mL in the S2AI group). In another single-center study by Elder et al33 of 90 patients (25 patients in the iliac screws group and 65 in the S2AI group), authors found that the iliac screws group had higher rates of reoperation (48.0% vs 8.8%, P < 0.001), surgical site infection (44.0% vs 1.5%, P < 0.001), wound dehiscence (36.0% vs 1.5%, P < 0.001), and symptomatic screw prominence (12.0% vs 0%, P = 0.02). On the other hand, they found that the rates of L5-S1 pseudarthrosis, proximal junctional failure, and sacroiliac joint pain were the same in both groups. Pain relief and functional recovery were achieved in both groups without significant intergroup differences. In their multivariate analysis, they found that younger age and the use of S2AI screws were protective of reoperation. Finally, they concluded that the use of S2AI screws over the conventional iliac screws was an independent predictor of preventing reoperation and surgical wound infection while achieving similar clinical and functional outcomes.
CONTEMPORARY ADVANCES IN SACROPELVIC FIXATION AND FUTURE PROSPECTS
The increasing advancements of technological applications in spine surgery aim toward maximizing patient safety, enhancing the technical aspect of the surgical procedure, and improving overall clinical outcomes. Currently, additional adjunct surgical modalities are being developed and tested with the aim of making SP fixation logistically and technically more feasible (eg, 3-dimensional patient-specific screw template guide, augmented reality-navigated S2AI screw insertion, and robotic-assisted screw placement).13,47
Shillingford et al have performed a propensity-matched analysis to assess the accuracy of freehand insertion vs robotic-assisted placement of S2AI screws.48 Their analysis was performed on a total of 51 patients, and they found that there was no significant difference in the overall accuracy between freehand screws and the robotic-assisted S2AI screws (94.9% vs 97.8%, P = 0.6). Moreover, they reported no neurovascular or visceral complications associated with the S2AI screws placement. Bederman et al49 also investigated the feasibility of robotic-assisted S2AI screws in spinal deformity correction and reported the same results. The data available suggest that robotic-guided S2AI screw insertion is accurate and a feasible option for patients requiring SP fixation.49–51 To our knowledge, none of the available studies discussed robotic S2AI screw placement reported major complications, including visceral injuries.12,48,52 Nevertheless, larger studies are required to assess the feasibility of using robotic-guided S2AI screw insertion as a gold standard technique over the freehand technique.
CONCLUSION
SP fixation remains a challenging surgical procedure for spine surgeons. The choice of suitable surgical modalities to achieve proper fixation remains imperative. With the available wide spectrum of surgical techniques used in SP fixation, the available data point toward the clinical advantage of S2AI screws on multiple fronts when compared with the conventional iliac screws (postoperative infection, symptomatic screw prominence, instrument failure, rate of revision surgery, etc). Nevertheless, the newly emerging data discussing the clinical outcomes of the subcrestal iliac screw technique and how it requires less complex instrumentation construct as these screws eliminate the need for an offset connector placement and results in lower rates of screw head prominence. In our experience, the subcrestal iliac screw technique represents a safe, feasible, and reliable method of pelvic fixation. The literature dedicated to comparing iliac screws and S2AI screws remains scarce, and the ability to determine whether S2AI screws are the superior surgical modalities for patients requiring pelvic fixation needs further validation.
Acknowledgments
The authors thank BodyParts3D, © The Database Center for Life Science licensed under CC Attribution-Share Alike 2.1 Japan, (DBCLS), for providing the images used in creating the Figures.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests Dr. Agarwal discloses royalties from Thieme Medical Publishers and serves as a consultant for Springer International Publishing. All remaining authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest in the subject matter or materials discussed in this manuscript.
Ethics Approval This study was approved by the University of Pittsburgh Institutional Review Board: REN15040166.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.