


Abstract
Background In anticipation of Food and Drug Administration (FDA) approval of the Total Posterior Spine (TOPS) system, the International Society for the Advancement of Spine Surgery (ISASS) conducted a study to estimate the work relative value units (RVUs) for facet arthroplasty. The purpose of this study was to establish a valuation of work RVU for Current Procedural Terminology (CPT) Code 0202T in the interim until the Relative Value Scale Update Committee (RUC) can determine an appropriate value. The valuation established from this survey will assist surgeons to establish appropriate procedure reimbursement from third-party payers.
Methods A survey was created and sent to 52 surgeons who had experience implanting the TOPS system during the investigational device exemption clinical trial. The survey included a patient vignette, a description of CPT Code 0202T along with a video of the TOPS system, and a confirmation question about the illustration’s effectiveness. Respondents were asked to compare the work involved in CPT Code 0202T to 8 lumbar spine procedures. A Rasch analysis was performed to estimate the relative difficulty of CPT 0202T using the work RVUs of the comparable procedures.
Results Forty-one surgeons responded to the survey. Of all the procedures, CPT Code 0202T received the most responses for equal work compared with posterior osteotomy (46%) followed by transforaminal lumbar interbody fusion (41%). The results of the regression analysis indicate a work RVU for CPT 0202T of 39.47.
Conclusion The study found an estimated work RVU of 39.47 for CPT Code 0202T using Rasch analysis. As an alternative to this Rasch methodology, one may consider a crosswalk methodology to the work RVUs for transforaminal lumbar interbody fusion procedurally, not as an alternative code.
Clinical Relevance These recommendations are not a substitute for RUC methodology but serve as a reference for physicians and third-party payers to understand work RVU similarities for charge and payment purposes temporarily until RUC methodology provides accurate RVUs for the procedure.
Level of Evidence 4.
INTRODUCTION
The concept of facet arthroplasty was first explored in clinical settings in the early 2000s with technologies such as Total Facet Arthroplasty System (TFAS), Acadia, and the original Total Posterior Spine (TOPS) system. All 3 underwent investigational device exemption (IDE) studies beginning in 2005, and all 3 were terminated early. TFAS and Acadia were metal-on-metal designs, which were halted in 2009 and 2011, respectively. The original TOPS IDE was halted due to a lack of funding. Premia Spine acquired the intellectual property for the TOPS system in 2012 and redesigned the implant to make it smaller. Commercial distribution outside the United States was started in 2013 with the redesigned TOPS. The US IDE was started in 2017 and concluded with US Food and Drug Administration (FDA) approval on 15 June, 2023.1 The TOPS system is the only facet arthroplasty device to complete a clinical trial and to be approved for commercial use. TOPS as a facet arthroplasty solution has been in clinical development for 18 years when considering the original IDE in 2005.
The American Medical Association (AMA) implemented Current Procedure Terminology (CPT) code 0202T, defined as, “posterior vertebral joint(s) arthroplasty (eg, facet joint[s] replacement), including facetectomy, laminectomy, foraminotomy, and vertebral column fixation, injection of bone cement, when performed, including fluoroscopy, single level, lumbar spine,” in 2010 to describe posterior vertebral joint arthroplasty. This is the code representative of the procedure performed utilizing the TOPS system.2 However, because this is a Category III code (temporary codes for emerging technologies), there is no current work relative value unit (RVU) assigned to this procedure. The present study aims to establish a valuation in work RVUs for posterior vertebral joint arthroplasty by Rasch analysis. The valuation of work RVUs developed by this analysis is not to undermine RUC methodology but rather to be used as a temporary estimate of work RVUs to establish charges and third-party payment until the RUC can determine an appropriate value. The International Society for the Advancement of Spine Surgery (ISASS) collected data from surveys distributed to TOPS US IDE orthopedic spine surgeon and neurosurgeon investigators. These surveys assessed the intricacies involved in performing a posterior vertebral joint arthroplasty in direct comparison to analogous surgical procedures.
Lumbar spinal stenosis (LSS) is caused by the narrowing of the central canal, nerve root, and intervertebral canals due to degenerative changes.3 An estimated 11% of the adult population has LSS, and the number is growing as the population ages.4 Currently, there is no single surgical procedure to address all spinal stenosis pathologies.5 LSS surgical treatment options include indirect decompression via interspinous distraction devices or lateral interbody, direct decompression, direct decompression with interlaminar stabilization, and direct decompression with fusion.5 TOPS treats LSS via direct decompression (open laminectomy) with multiaxial, posterior stabilization (it has been cited as a 3-column stabilizer).6 Per the FDA, indications for use of the TOPS procedure are as follows: “Patients between 35 and 80 years of age with symptomatic degenerative spondylolisthesis up to Grade I, with moderate to severe lumbar spinal stenosis and either thickening of the ligamentum flavum and/or scarring of the facet joint capsule at one level from L3 to L5.”1
Preparations for this study were initiated in April 2023 in anticipation of FDA approval. Our study was conducted using an ISASS-established Rasch method protocol.7 Neurosurgeon Robert A. Florin, an experienced past member of the RUC, has not only endorsed but also validated the Rasch methodology.8 Florin effectively harnessed this approach to assess the relative workloads associated with various health care procedures, establishing its credibility in the medical field.9 Furthermore, Rasch methodology expands beyond health care. In the sphere of education, it plays a crucial role in gauging the relative difficulty of individual test items, ensuring fair evaluations.10 In the dynamic world of marketing, it is instrumental in discerning consumer preferences among different products.11 Additionally, in the domain of health economics, Rasch methodology serves the purpose of assessing the desirability of various health states, including medical conditions.12 Its versatility and applicability underscore its significance across a spectrum of disciplines.
The Rasch method for assessing health care procedures involves a systematic approach utilizing paired comparisons. In a conventional Rasch analysis, each CPT code within a specific category is paired with every other code within that same category. Respondents then express which of the paired procedures they believe demand a greater degree of work effort. Subsequently, sophisticated logistic regression techniques come into play to calculate the likelihood that one procedure requires more effort compared with the others. These calculations also help establish a numerical representation of the procedure’s difficulty or work-effort score within the given set. These scores are expressed as logits, representing values on a cardinal scale. To provide a frame of reference, one procedure is arbitrarily assigned a score of 0.5.8 This cardinal scale stands apart from nominal scales (nominal scales do not have ordered classes, such as hair color [blonde, brunette, black, etc]) and ordinal scales (ordinal scales have an order, but no specific interval, such as education level [high school, bachelors, masters, etc]). Cardinal scales, on the other hand, not only maintain order but also feature a meaningful interval. Following the generation of these work-effort scores, the process continues by estimating RVUs through regression analysis, making use of the preexisting RVUs as a basis for these estimations. This comprehensive approach ensures a thorough evaluation of the relative complexities and work efforts associated with various medical procedures.
The surgical procedure performed with this emerging technology is “new” and may be considered complex compared with other motion preservation procedures that spine surgeons perform. The sole intent of the ISASS project is to perform a “Paired Comparison Survey to Determine the Work Valuation For CPT Code 0202T.” This validated survey using Rasch methodology will identify an “interim” surgeon work valuation based on a similar procedure. Interim is defined as an intervening period—provisional or temporary. A Rasch analysis, which is not RUC methodology, supports the following intentions: (1) use as an interim tool before Category I CPT code valuation is established, (2) offer rationale to assist with procedure crosswalk for third-party payer reimbursement, (3) support member’s procedure valuation for payment without bias, and (4) provide validated methodology as requested by third-party payers.
METHODS
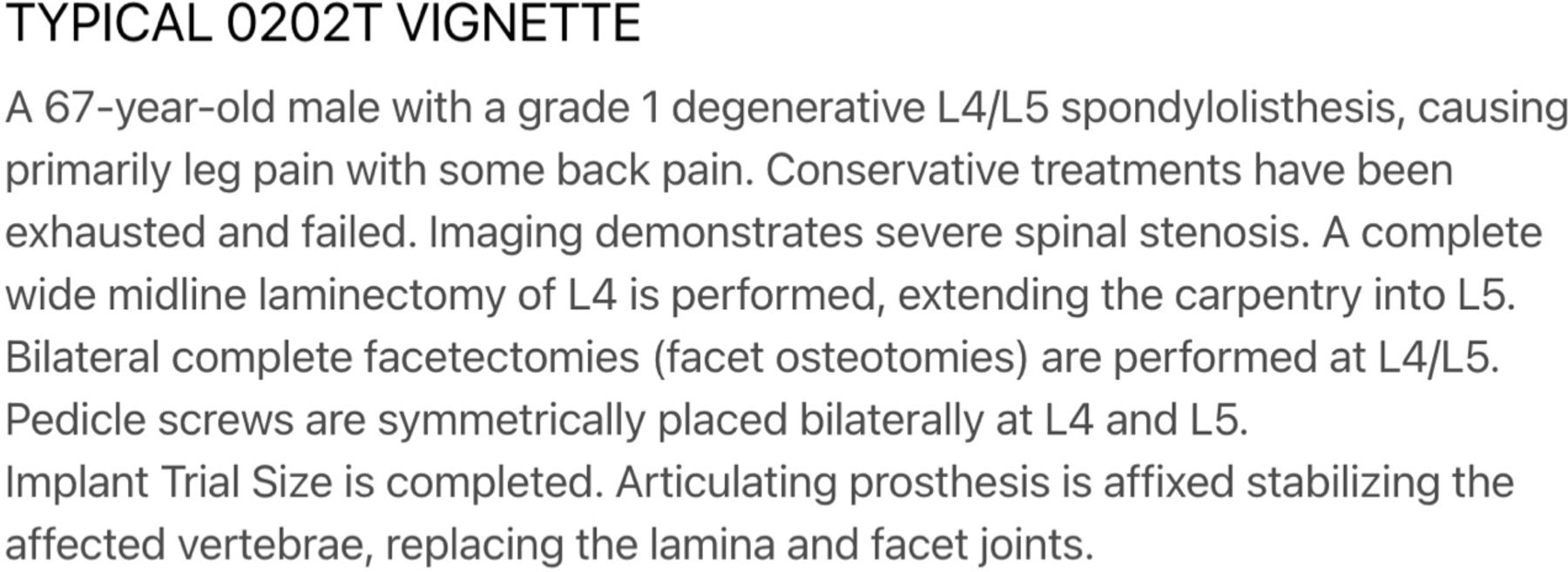
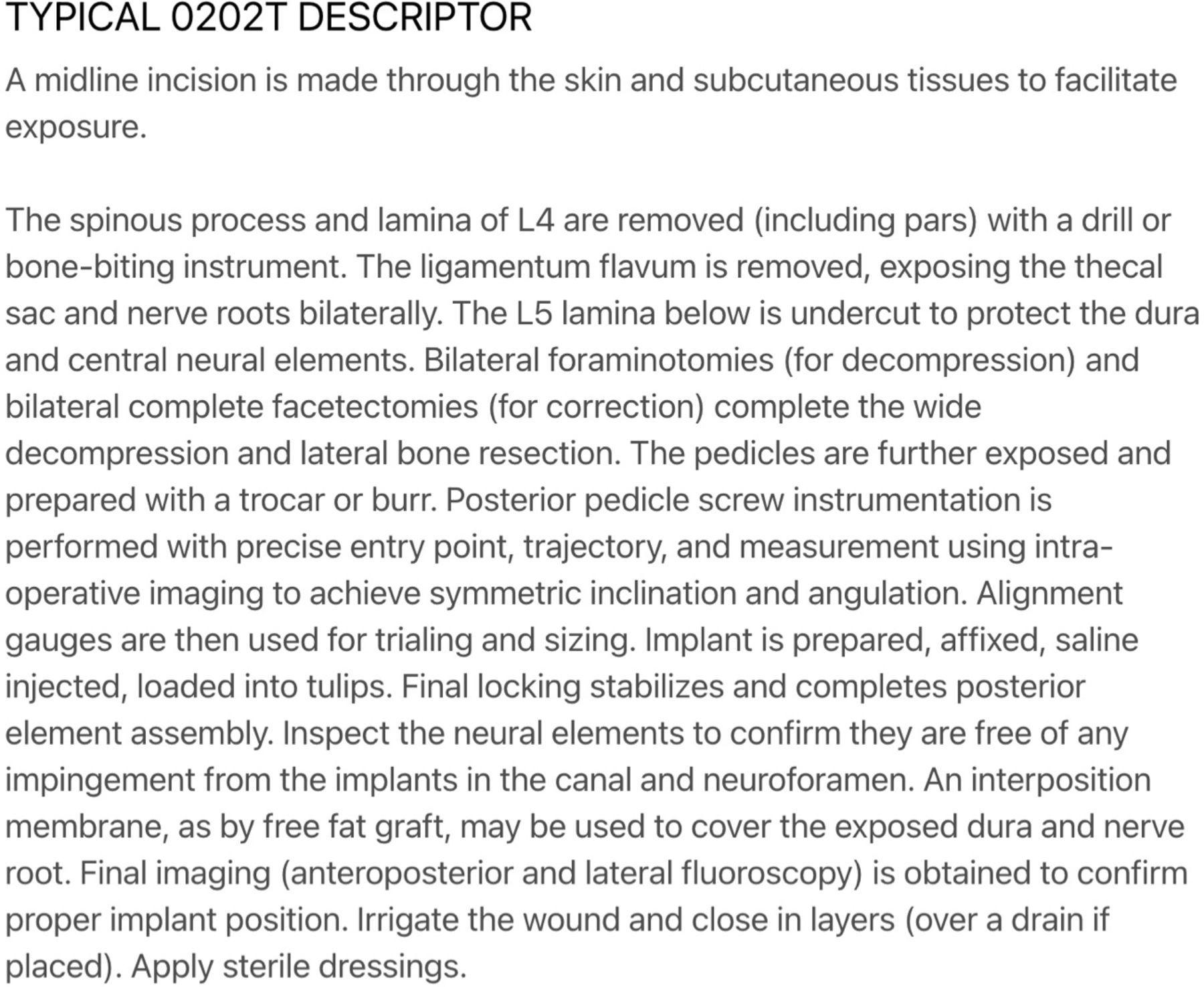
Using Typeform, a survey was created to be analyzed using the Rasch method. This study was approved by ISASS executives at the May 2023 ISASS Board of Directors Meeting. The survey was sent to all 52 TOPS US IDE surgeon investigators—including orthopedic spine and neurosurgeons—on 30 July, 2023 by the ISASS Coding and Reimbursement Task Force. Responses were concluded on 12 August, 2023. A total of 41 surveys were completed. The survey gathered data on whether surgeons had performed the procedure and their primary practice location, primary specialty, and professional memberships. A patient vignette was shown describing a standard LSS patient (Figure 1). Following the vignette, a description of CPT Code 0202T was provided with an associated video of the TOPS system (Figure 2, Online Supplemental Video 1). A confirmation question stating, “Is the illustration a helpful tool in demonstrating the work and complexity of the procedure to support the physician work involved in the TOPS procedure?” was prompted following the video. Eight posterior lumbar spine procedures that would be recognized as familiar (or well known from long association to spine surgeons) were listed with responses, including that 0202T requires less physician work, more physician work, equal physician work, and not applicable (for physicians who do not perform the procedure).

Patient vignette for CPT Code 0202T prompted in the survey.

Descriptor of CPT Code 0202T presented following the vignette in the survey.
Unlike historic Rasch methodology, our survey included comparable procedures, not specific comparable CPT codes. This methodology was used due to CPT Code 0202T being a bundled procedure code, requiring bundled procedure comparisons that were facilitated via building block methodology where appropriate. For example, transforaminal lumbar interbody fusion (CPT Code 22630) alone is not a comparable procedure to CPT Code 0202T. Since a single CPT Code is not a sufficient comparator alone, our survey asked CPT Code 0202T work to be compared with, “Transforaminal lumbar interbody fusion; 1 interspace (CPT Code 22630)—with posterior nonsegmental instrumentation (CPT Code 22840)—with insertion of interbody device (CPT Code 22853)—with placement of spine [local] autograft (CPT Code 20936).” Similar bundled procedures were included for 5 of the remaining 7 procedures seen in Table 1. The bundling technique and work RVU valuation for the comparison procedures can be found in Supplemental Table 1. Our survey was analyzed by an outside, independent professional CPT coding party to ensure appropriate use of codes chosen and/or use of modifiers where appropriate. The work RVUs selected were taken from the 2023 Medicare Physician Fee Schedule.
Procedures and CPT codes used in the survey.
Responses to the survey were coded 0 if CPT Code 0202T was less work than the comparison procedure and 1 if CPT Code 0202T was more work than the comparison procedure. Responses stating CPT Code 0202T was equivalent to the comparison procedure were assigned randomly to 0 or 1 at a 1:1 ratio. This was done to mitigate survey noise while accounting for equivalent work procedures, as equivalent is not the same as no response.
Statistical Methods
The Rasch analysis was conducted in Jamovi, a statistical software. The Rasch analysis estimated the difficulty scores for each procedure relative to CPT 0202T. Simple linear regression of difficulty scores and bundled procedure work RVUs were performed. A best-fit line correlating estimated work RVUs with increasing difficulty scores was generated. Work RVUs for CPT 0202T were found using the line of best-fit formula with a difficulty score of 0. Responses of surgeon type and relative difficulty of CPT 0202T to each bundled procedure were assessed as categorical variables. Pearson’s chi-square test was used for the analysis of categorical variables. IBM SPSS Statistics v29.0 (Armonk, NY, USA) was utilized for statistical analysis. Significance was defined as a P value ≤0.05.
RESULTS
Demographics
A total of 41 physicians responded to the survey (52 surgeons were contacted for a response rate of 79%). All respondents reported performing the procedure associated with CPT Code 0202T previously. The most common primary practice location was urban (60%), followed by suburban (21%) and rural (19%). The most common specialty was neurosurgery (50%), followed by spine (33%) and orthopedics (17%). The most common associated professional organization among respondents was the American Association of Neurological Surgeons (61%), followed by the Congress of Neurological Surgeons (51%), the North American Spine Society (44%), ISASS (42%), the American Academy of Orthopaedic Surgeons (29%), the AMA (24%), and the Society of Minimally Invasive Spine Surgery (15%).
Of all the procedures, CPT Code 0202T received the most responses for equal work compared with posterior column, Smith-Peterson (Ponte), and osteotomy (46%), followed by transforaminal lumbar interbody fusion (41%) and posterior arthrodesis for spinal deformity up to 6 vertebral segments (27%). CPT Code 0202T received the most responses for more physician work compared with the insertion of interlaminar stabilization device without fusion (68%), followed by laminectomy (65%) and posterior/posterolateral arthrodesis 1L (63%). CPT Code 0202T received the most responses for less physician work compared with posterior arthrodesis for spinal deformity of 7–12 vertebral segments (68%), followed by posterior arthrodesis for spinal deformity up to 6 vertebral segments (41%). Surgeons in rural locations were significantly more likely to report that CPT Code 0202T was more work than posterior osteotomy compared with suburban and urban physicians (86% vs 22% vs 32%, P = 0.016). There was no significant difference in responses between neurosurgeons, orthopedic surgeons, and spine surgeons for all procedures (Supplemental Table 2).
Estimated Work
Survey responses to the procedures listed in Table 1 were used for the Rasch analysis. The output of the analysis is shown in Table 2. Each procedure is listed with an estimated difficulty score relative to CPT Code 0202T. CPT Code 0202T has a score of 0. Negative difficulty scores indicate that CPT Code 0202T is more difficult and positive difficult scores indicate that CPT Code 0202T is less difficult.
Difficulty scores estimated by the Rasch analysis.
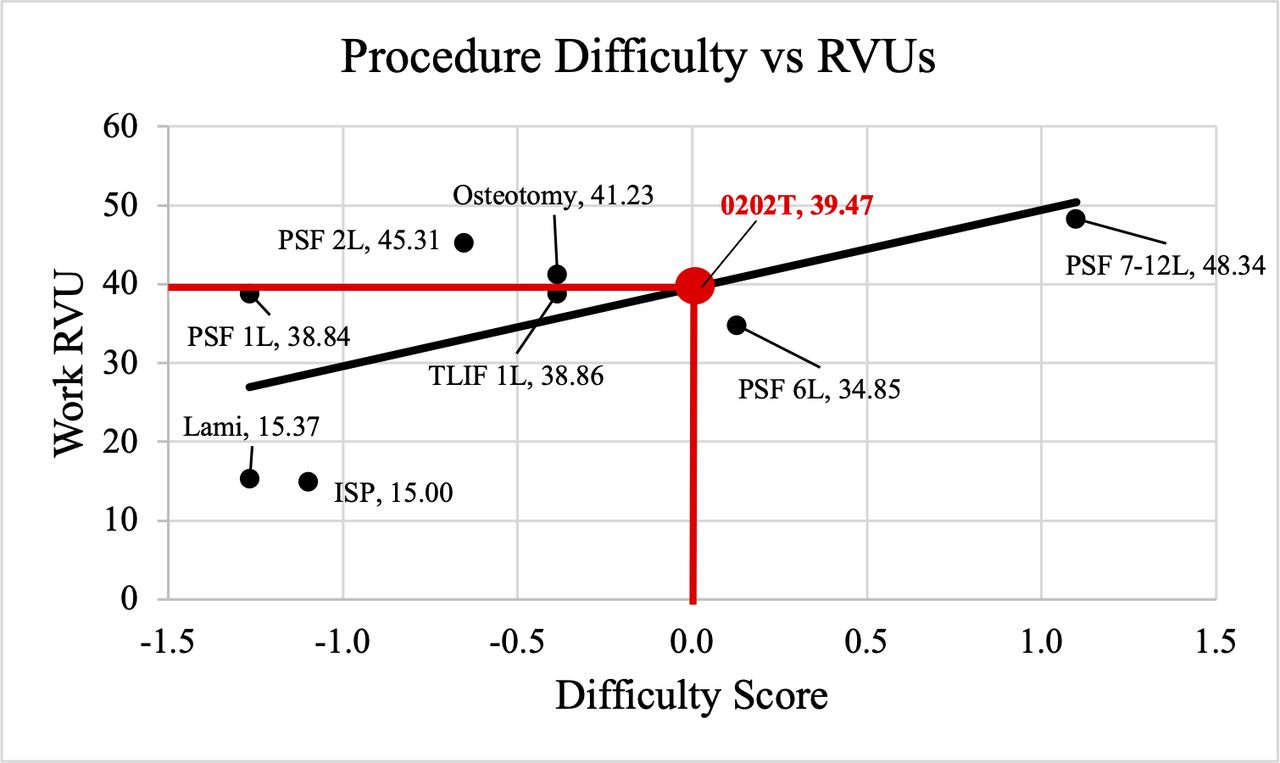
The work RVUs from Table 1 and the difficulty scores from Table 2 were analyzed by simple linear regression. Regression analysis of difficulty score (independent variable) and work RVUs (dependent variable) has an estimated intercept of 39.47 and a slope of 9.92. Using the equation work RVUs = intercept + slope × difficulty, the estimated work RVU for CPT Code 0202T is 39.47 because difficulty of CPT Code 0202T would be a value of zero. Figure 3 shows the results of the analysis. Points are labeled as their procedure and work RVUs. Approximately 40% of the variation in work RVU was explained by the work of the procedure found in the linear regression (R 2 = 0.39).
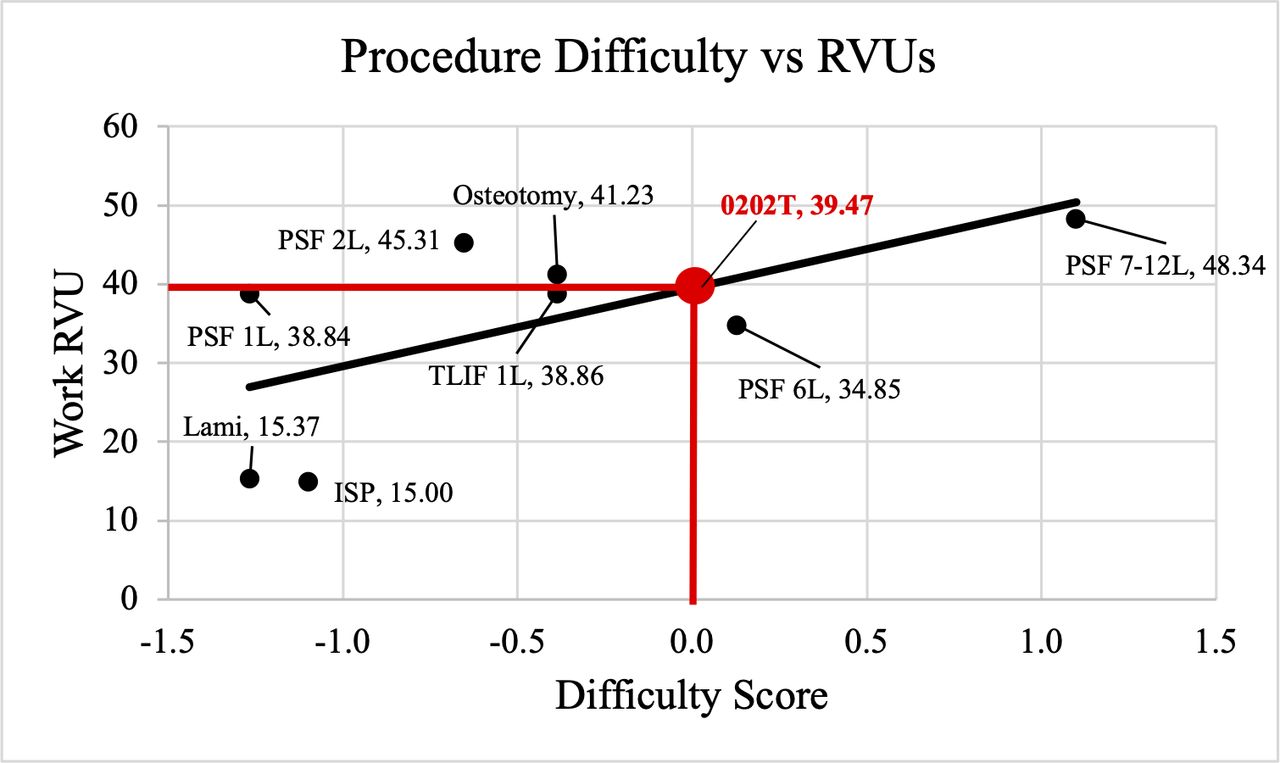
Results of regression analysis to estimate relative value units for CPT Code 0202T. ISP, interlaminar stabilization device without fusion; Lami, laminectomy; Osteotomy, posterior osteotomy; PSF 1L, posterior/posterolateral arthrodesis 1L; PSF 2L, posterior/posterolateral arthrodesis 2L; PSF 6L, posterior arthrodesis for spinal deformity up to 6 vertebral segments; PSF 7–12L, posterior arthrodesis for spinal deformity 7–12 vertebral segments; TLIF, transforaminal lumbar interbody fusion.
DISCUSSION
In 1992, the Centers for Medicare & Medicaid Services (CMS) introduced the Medicare Physician Fee Schedule, which brought about a standardized payment system. This system, overseen by CMS, serves as a reference point for private health insurers when negotiating payment agreements with healthcare providers. To aid in this process, the Relative Value Scale Update Committee (RUC) was established in 1991, functioning as an expert panel tasked with formulating recommendations on relative value for CMS. The determination of procedure code values involves the amalgamation of 3 key components: work, practice expenses, and malpractice expenses (Total RVU = Work RVU + Practice Expense RVU + Malpractice Expense RVU). The calculation of the work RVU relies on factors such as time and intensity, drawing upon research conducted by Hsiao et al at Harvard University.13
Evaluating the effort expended in medical work is a somewhat subjective endeavor. Time serves as the primary, and most objectively measurable, factor when assessing a physician’s workload. In contrast, gauging intensity introduces a greater degree of subjectivity and encompasses factors such as technical skill and physical exertion, mental effort and decision-making, and emotional stress and strain. The work RVU further dissects this into 3 categories: preservice work, intraservice work, and postservice work. These divisions are determined through a rigorous process that involves surveys conducted by the RUC, capturing insights into the time and intensity required to complete a given medical procedure. It is worth noting that intraservice work often exhibits the most variability in terms of intensity among these categories.14
In the context of spine procedure coding and bundle assessments, differentiating between Rasch analysis and the crosswalk methodology is crucial. The crosswalk approach, akin to a Venn diagram, identifies commonalities between codes and procedures, while Rasch analysis, founded on the Rasch model, excels in precision.15 It operates on the principle that a person’s ability to understand or perform a medical procedure correlates with the procedure’s difficulty, offering insights adaptable to specific research contexts.16 Rasch analysis, addressing construct validity through fit statistics and item-person map gaps, provides a level of internal validity that remains independent of the sample to which it is applied.17,18 This ensures that findings can accurately extrapolate to a broader population, making Rasch analysis a valuable tool for granular evaluation of CPT codes and bundled procedures in spine research and clinical practice.
Category III codes, being for “emerging technologies, services, and procedures,” do not undergo RUC survey; thus, there is currently no work RVU assigned to CPT Code 0202T by the RUC. Our study produced an estimated work RVU for CPT Code 0202T of 39.47. When examining procedures thought by surgeons to be most similar in the amount of work (posterior osteotomy, transforaminal lumbar interbody fusion, and posterior arthrodesis for spinal deformity up to 6 vertebral segments), the average work RVU is 38.31. This value is very close to the work RVU valuation for transforaminal lumbar interbody fusion (38.86). Thus, crosswalk methodology to transforaminal lumbar interbody fusion procedurally may be an appropriate alternative to this modified Rasch analysis in this instance. Historically, the North American Skull Base Society created a document using crosswalk methodology for endoscopic skull base surgery since there is no CPT Code that appropriately describes the work.19
This study was not without limitations. First, due to the binary requirement of the Rasch analysis, one cannot analyze results with 3 categories. To account for this, randomization of the equal work into a category of more work or less work was done in a 1:1 ratio. In addition, the fact that CPT Code 0202T is a bundled procedure code being compared to other procedures with multiple CPT codes could be seen as a limitation. We accounted for this by having our bundled procedures assessed for validity and accuracy by an outside professional CPT coder. Finally, the RUC survey relies heavily on the time and intensity of the procedure, while the Rasch analysis relies on a surgeon’s perception of work.
The purpose of this study was to determine an estimated work RVU for physicians to be aware of in relation to comparable spinal procedures.The ISASS Coding and Reimbursement Task Force conducted this study to prevent underutilization of posterior vertebral joint(s) arthroplasty until the RUC determines the appropriate procedural work RVU.
CONCLUSION
The results of our study yielded an estimated work RVU of 39.47 for CPT Code 0202T via Rasch analysis. Crosswalk methodology, a common but potentially misvalued alternative to Rasch methodology, may be considered when no other statistical method is available. A crosswalk might assign 0202T the same work RVUs as transforaminal lumbar interbody fusion if the surgeon, at their discretion, opts for the comparable bundled TLIF procedure as most appropriate. This would be for procedure valuation only and not as a substitute code. Our recommendations are not to be used as a substitute for RUC methodology in determining RVUs for procedures but are to be used by the physicians to see the similarities of work RVUs between CPT Code 0202T and comparable spinal procedures. Physicians can utilize this analysis and the concluded valuation for reimbursement purposes at their discretion in the interim that RUC methodology produces the appropriate RVUs for this procedure.
Supplementary material
Supplemental Table 2.
Physician survey responses comparing bundled procedures to CPT Code 0202T.SupplementalTable2_CPT0202T.doc
Online Supplemental Video 1.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosures J.Y. reports royalties/licenses from Aesculap Spine; consulting fees and payment/honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Aesculap Spine and Abbott Labs; payment for expert testimony from various legal firms; and participation on a data safety monitoring board or advisory board for Medtronic Spine and Intrinsic Therapeutics. M.L., K.-U.L., K.H., R.K., and J.Y. are unpaid, voluntary members of the ISASS Coding and Reimbursement Task Force.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.