


Abstract
Background The International Society for the Advancement of Spine Surgery hosted the third in a series of webinars focused on innovative endoscopic spine surgery techniques. This session aimed to discuss and evaluate advanced treatments for lumbar spinal stenosis and related conditions utilizing multiportal endoscopic approaches; articulating instruments; unilateral biportal endoscopy; transforaminal techniques for facet cysts, herniated disc, and spinal stenosis; as well as percutaneous endoscopic lumbar interbody fusion (PELIF).
Objective To analyze the level of surgeon endorsement for the presented endoscopic spine surgery techniques before and after the webinar, utilizing polytomous Rasch analysis, and to evaluate the potential for these insights to inform clinical guideline recommendations.
Methods An online survey was administered to 868 surgeons during a sponsored webinar hosted by the International Society for the Advancement of Spine Surgery. The survey used Likert-scale ratings to evaluate 5 main topics and additional surgical experiences and was distributed before and after the webinar. Survey responses were analyzed using descriptive statistics and Polytomous Rasch analysis to evaluate shifts in acceptance and perception.
Results Of the 793 surgeons who attended the webinar, 229 accessed the prewebinar survey, 154 began it, and 119 completed it, yielding a completion rate of 77.3%. The respondents included 52.9% orthopedic surgeons, 37.0% neurosurgeons, 1.7% fellows, 0.8% residents, and 0.8% medical students. In the postwebinar phase, engagement remained high, with 298 accessing the survey, 169 starting it, and 128 completing it, resulting in a 75.7% completion rate. The postwebinar participant demographics closely resembled the initial distribution, consisting of 53.1% orthopedic surgeons, 35.9% neurosurgeons, 6.2% residents, 3.1% fellows, and 1.6% medical students. The confidence in various endoscopic techniques saw notable changes, particularly for procedures involving transforaminal lateral canal decompression for stenosis, herniated disc, and low-grade spondylolisthesis. Unilateral biportal endoscopy facet joint decompression and PELIF saw an increase in high-level endorsements after the webinar. Polytomous Rasch analysis provided insights into procedural techniques. The study showed consensus on the effectiveness of percutaneous endoscopic decompression of low-grade spondylolisthesis, reflecting evolving surgeon preferences and consensus on best practices. Infit and outfit statistics from the Rasch analysis suggested a good fit between the survey responses and the Rasch model both before and after the webinar, indicating minimal data distortion due to bias except for transforaminal decompression for posterolateral and central herniated nucleus pulposus. Differential item functioning analysis showed no significant bias in item responses between orthopedic surgeons and neurosurgeons in the prewebinar survey but identified potential bias for 1 item postwebinar in PELIF and articulating instruments.
Conclusion The webinar influenced surgeon perceptions and endorsements of advanced endoscopic techniques, substantially impacting professional practice. Continued use of Rasch analysis in evaluating educational interventions offered a nuanced understanding of changes in surgical practice toward more complex and controversial issues such as central and migrated herniated nucleus pulposus, facet cyst, low-grade spondylolisthesis, and fusion while potentially guiding future clinical guidelines and training programs to align with evolving endoscopic techniques.
Clinical Relevance Assessing surgeon confidence and acceptance of endoscopic spinal surgeries using polytomous Rasch analysis.
Level of Evidence Level 2 (inferential) and 3 (observational) evidence because Rasch analysis provides statistical validation of instruments rather than direct clinical outcomes.
- endoscopic spine surgery
- polytomous Rasch analysis
- surgeon endorsement
- unilateral biportal endoscopy (UBE)
- percutaneous endoscopic lumbar interbody fusion (PELIF)
- transforaminal discectomy
- facet cyst
- clinical guidelines
Introduction
The International Society for the Advancement of Spine Surgery (ISASS) recently hosted the third webinar of a 4-part series on cutting-edge endoscopic spine surgery techniques. This session aimed to disseminate knowledge and encourage discussion regarding innovative treatments for lumbar spinal stenosis. It highlighted the utility of simultaneous multiportal endoscopic strategies for complex lumbar conditions, the benefits of articulating instruments, and the use of percutaneous endoscopic lumbar interbody fusion (PELIF) with supplemental posterior non-segmental pedicle instrumentation. Additional topics included unilateral biportal endoscopy (UBE) decompression for lumbar facet cysts, treatment of low-grade spondylolisthesis, and managing a variety of painful lumbar conditions using transforaminal endoscopic decompression ranging from lateral and central canal stenosis to posterolateral, migrated, and central herniated nucleus pulposus (HNP) to facet cyst decompression.
Insights from the session were gathered through surveys conducted before and after the event and analyzed using polytomous Rasch analysis to gauge participant acceptance of each discussed topic and procedure.1–8 Furthermore, incorporating the Rasch model, based on item response theory (IRT), this approach provides a sophisticated framework for analyzing response data from the series. The Rasch logistic response model focuses on the relationship between individuals’ abilities (or trait levels) and the difficulty of items within a measurement instrument. Therefore, the application of Rasch analysis frees the comparison of item difficulties across groups from differences in the distribution of person ability within groups. It specifies a logistic transformation of the traditional item difficulties as the only reasonable transformation. The variance of item difficulty estimates now corresponds to the real situation in which information is maximum in the center and minimum at the extremes. By effectively addressing the probabilistic elements of decision-making and aligning task difficulty with individual proficiency, the Rasch model is ideal for dissecting agreement levels on the topics discussed.8
Spine surgery poses unique challenges that are not fully captured by traditional statistical methods for analyzing patient-reported outcomes or surgical decisions. The Rasch model overcomes these challenges and offers several benefits by treating categorical data like Likert-scale responses with mathematical rigor. It provides a nuanced understanding by assessing the complexity of decisions in the context of a surgeon’s expertise, transforms ordinal data into a precise interval-level scale for more accurate comparisons, ensures consistent measurement across different surgical decisions for reliable comparisons, identifies outliers to refine tools for evaluating surgical judgment, and fosters improvements in educational and guideline development by highlighting areas of strength and weakness in decision-making, ultimately enhancing surgical outcomes. This approach offered a detailed analysis of participant perceptions, experiences, and outcomes, establishing a strong foundation for evaluating the effectiveness of these endoscopic techniques and the satisfaction levels of surgeons. The Rasch model converts the expertise shared during the webinar into actionable insights for assessing clinical evidence based on surgeon feedback. The results could play a significant role in shaping clinical guidelines for endoscopic spine surgery.
Materials and Methods
Webinar and Surgeon Survey
The authors disseminated an online questionnaire through www.typeform.com to 793 potential surgeon participants using a link shared during the ISASS-sponsored Zoom webinar on 2 April 2024. Participants were requested to rate their support or the significance they placed on the 4 topics discussed at the webinar. Ratings were given on a Likert scale ranging from 1 to 5, with 1 signifying low and 5 high. This assessment was conducted at the beginning and end of the webinar to gauge changes in the participants’ levels of endorsement resulting from the lectures presented. The manuscript’s authors introduced the following 4 topics (Figure 1):
“The Benefit of Simultaneous Multiportal Endoscopic Approaches and Articulating Instruments” by Choll Kim, MD, PhD, Excel Spine Center UCSD, Medical Center East Campus, Minimally Invasive Center of Excellence, San Diego, California, USA.
“Biportal Endoscopic Treatment of Lumbar Facet Cysts” by Brian Kwon, MD, New England Baptist Hospital, Assistant Clinical Professor of Orthopedic Surgery at Tufts University School of Medicine, Boston, Massachusetts, USA.
“Managing Low-Grade Spondylolisthesis With Endoscopic Spine Surgery” by John Ongulade, DO, Department of Neurological Surgery, Washington University School of Medicine, St. Louis, Missouri, USA.
“Percutaneous full endoscopic lumbar interbody fusion PELIF” by Kenyu Ito, MD, Aichi Spine Institute, Fuso-cho Niwa-gun, Aichi, 480–0102, Aichi Prefecture Chūbu, Honshū, Japan.

Left to right: Webinar moderator was Kai-Uwe Lewandrowski, MD; Faculty who presented on the following topics were as follows: (1) Kenyu Ito, MD, Aichi Spine Institute, Japan, presented “Percutaneous Full Endoscopic Lumbar Interbody Fusion.” (2) Choll Kim, MD, PhD, Excel Spine Center UCSD, San Diego, California, USA, presented ”The Benefit of Simultaneous Multiportal Endoscopic Approaches and Articulating Instruments.” (3) Brian Kwon, MD, New England Baptist Hospital, Boston, Massachusetts, USA, presented “Biportal Endoscopic Treatment of Lumbar Facet Cysts.” (4) John Ongulade, DO, Department of Neurological Surgery, Washington University School of Medicine, St. Louis, Missouri, USA presented, “Managing Low-Grade Spondylolisthesis With Endoscopic Spine Surgery.”
Additionally, survey participants were asked about their experience and clinical outcomes with transforaminal endoscopic decompression for lateral and central canal stenosis to posterolateral, migrated, and central HNP and painful lumbar facet cysts. Respondents also provided details about their postgraduate education.
Statistics and Rasch Analysis
The data were exported to Excel and analyzed with IBM SPSS (version 27) and Jamovi (version 2.3). Descriptive statistics were used to summarize responses and calculate means, ranges, SDs, and percentages. The χ 2 test assessed the relationship between variables, while the IRT module in Jamovi facilitated the Rasch analysis. A P value of less than 0.05 was considered statistically significant, and a 95% confidence interval was applied to all statistical tests. The polytomous Rasch model, as detailed in the Part 1 report and outlined by Andrich, was utilized in this survey of surgeons. This model suggests that the characteristics of both the individual and the item determine the probability of a specific outcome in an empirical context. It models ordered response data by the likelihood of a response falling into categories such as “strongly agree,” “agree,” “disagree,” or “strongly disagree.” In the polytomous Rasch model, scoring x on an item indicates that an individual has surpassed x thresholds on a continuum while not surpassing the remaining m − x thresholds. Mathematically, the application of the Rasch model in this study is expressed as the log odds (or logit) of a person endorsing an item, reflecting the difference between the person’s ability or level of agreement and the item’s difficulty. The model uses χ 2 fit statistics, outfit, and infit to evaluate the data’s fit to the model. The findings from the polytomous Rasch analysis are visually presented in the Wright plot9 and through person-item map analysis.10
Sample Size
The Rasch model operates under a principle of balanced requirements; to achieve a stable measure of individuals, the number of items presented should match the number of participants required to calibrate those items accurately. This symmetry is critical in psychometrics, as it ensures the reliability of the measurements derived from the model. According to Azizan et al, administering a set number of items—say, 30—to an equal number of participants, when done under conditions of appropriate targeting and good model fit, is likely to produce statistically stable measurements.11 Specifically, measures obtained in this setup are expected to be stable within ±1.0 logits at a 95% confidence level. This balance helps enhance the precision of the Rasch model, making it a robust tool for assessing the likelihood of responses across a standardized scale. Moreover, the stability these parameters indicate is essential for validating the construct under investigation and ensuring that the data reflect true differences in the trait or ability being measured rather than variations due to measurement error or sample size limitations.
Bias Detection
Rasch analysis excels at identifying disturbances in data, including biases, by analyzing residuals—the differences between observed and model-predicted responses. It generates fit statistics for each item to gauge their alignment with Rasch model expectations. The outfit mean square error statistic, sensitive to outliers, measures deviations from model predictions as a ratio of observed to expected variance, where a value of 1.0 signifies perfect fit, values above 1.0 indicate noise, and values below 1.0 suggest overfit. In contrast, infit is a weighted version that lessens the impact of less informative responses. Misfitting items, indicated by infit and outfit statistics, may function differently across respondent subgroups and could signal bias, known as differential item functioning (DIF). This bias can appear when individuals with equivalent abilities but different backgrounds respond inconsistently to an item. The difNLR() and difORD() functions are used for detecting DIF in dichotomous and ordinal data, respectively.12
Visual tools like person-item interaction maps and Wright plots, along with item characteristic curves, are used to visually inspect item performance across groups and assess bias by examining both infit and outfit statistics.13 Acceptable ranges for infit and outfit values, generally between 0.6 and 1.4, indicate a lack of distortion in the data. Additionally, the MAPQ3 methodology, rooted in IRT analysis, with values of 0.3 or less also indicates an absence of data distortion. These tools assist in identifying items that may disproportionately affect certain subgroups. Rasch analysis, particularly adept at detecting latent traits and item bias, was deemed more sensitive than traditional regression or analysis of variance in this context. These analytical strategies were described in detail in the previous ISASS webinar Part 2 publication, where readers can find more comprehensive information regarding bias detection with the Rasch methodology.
Results
The third installment of the ISASS webinar series “Current and Emerging Techniques in Endoscopic Spine Surgery” drew an initial online attendance of 793 surgeons. The prewebinar survey was accessed by 229 participants, 154 of whom started it, and 119 completed it, achieving a 77.3% completion rate. The demographic breakdown included 52.9% orthopedic surgeons, 37.0% neurosurgeons, 1.7% fellows, 0.8% residents, and 0.8% medical students. Similar participation was observed in the postwebinar phase, with 298 accessing the survey, 169 starting it, and 128 completing it, resulting in a 75.7% completion rate. The postwebinar demographics mirrored the initial poll, featuring 53.1% orthopedic surgeons, 35.9% neurosurgeons, 6.2% residents, 3.1% fellows, and 1.6% medical students.
A polytomous Rasch analysis of the responses from this webinar provided valuable insights into the acceptance of various endoscopic spine surgery techniques before and after the session. This analysis included items deemed critical for determining the relevance and impact of the following procedural aspects:
simultaneous multiportal endoscopic approaches and articulating instruments
UBE decompression of lumbar facet cysts
low-grade spondylolisthesis with endoscopic spine surgery
PELIF
transforaminal endoscopic decompression for the following:
lateral canal stenosis
central canal stenosis
posterolateral HNP
migrated HNP
central HNP
painful lumbar facet cysts
Descriptive Statistics of Learning Curve Assessment, Clinical Outcomes, and Endoscopic Techniques
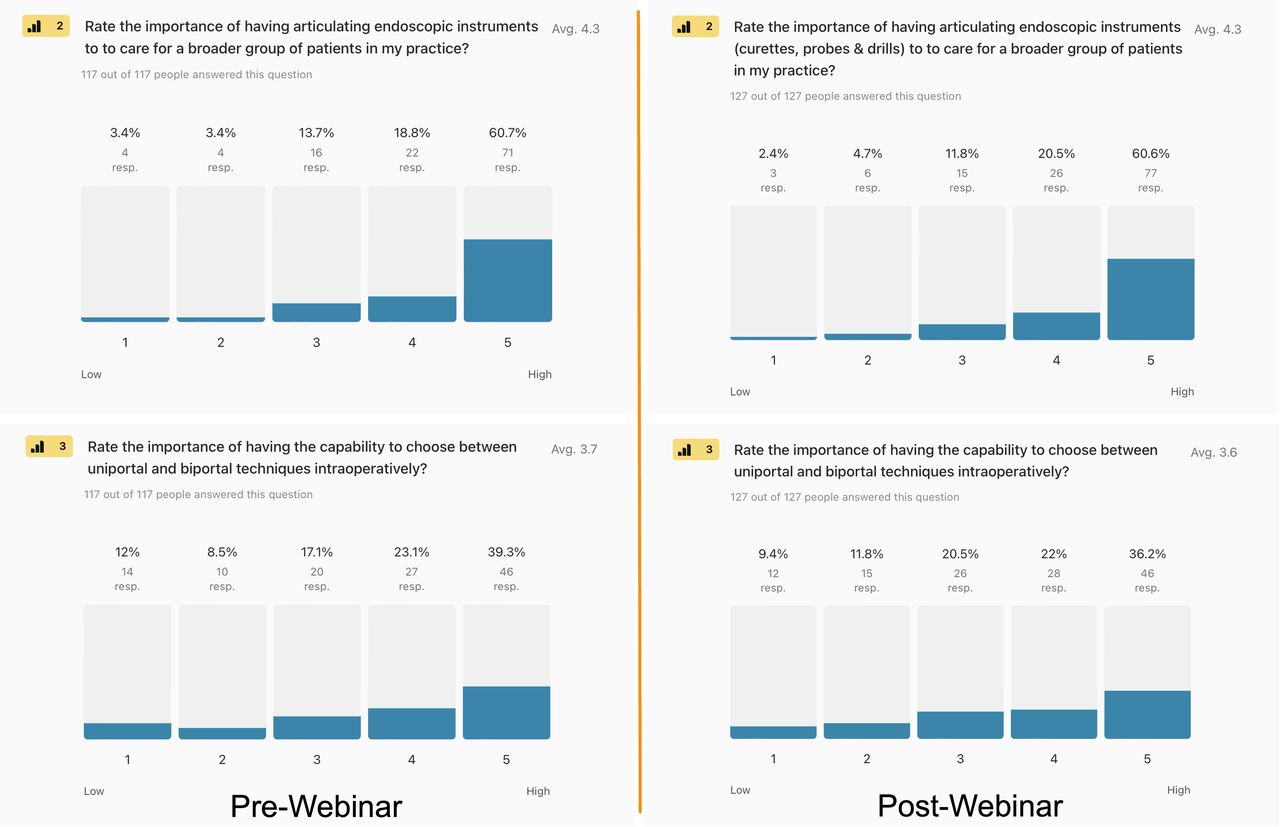
The descriptive statistics illustrated in Figures 2–4 reveal the changes in surgeons’ perceptions and endorsements of various endoscopic spine surgery techniques before and after the webinar. As depicted in Figure 2, articulating instruments in complex endoscopic decompression was endorsed by 79.4% of respondents before the webinar. The importance of articulating instruments was rated high (options 4 and 5 on a Likert scale), slightly increasing to 81.4% after the webinar. This opinion shift indicates a modest growth in recognition of these instruments’ significance in performing complex procedures. The data on multiportal technique flexibility (Figure 2) also represents the perceived advantages of switching between uniportal and biportal techniques during operations. Initially, 62.4% of surgeons saw this flexibility as beneficial. Still, this perception decreased to 58.2% in the postwebinar survey, suggesting possibly a slight shift in attitudes toward the value of technique versatility in a real-time surgical application or simply noise in the data.

Pre- and postwebinar descriptive statistics of the level of importance of having articulating instruments to perform complex endoscopic decompression spine surgery: (2) 79.4% of surgeons gave it the highest endorsement selecting options 4 and 5 on a Likert scale from 1 to 5 before the webinar vs 81.4% after the webinar. (3) Similarly, 62.4% of prewebinar and 58.2% of postwebinar respondents thought that switching between uniportal and biportal techniques during the same operation was advantageous.

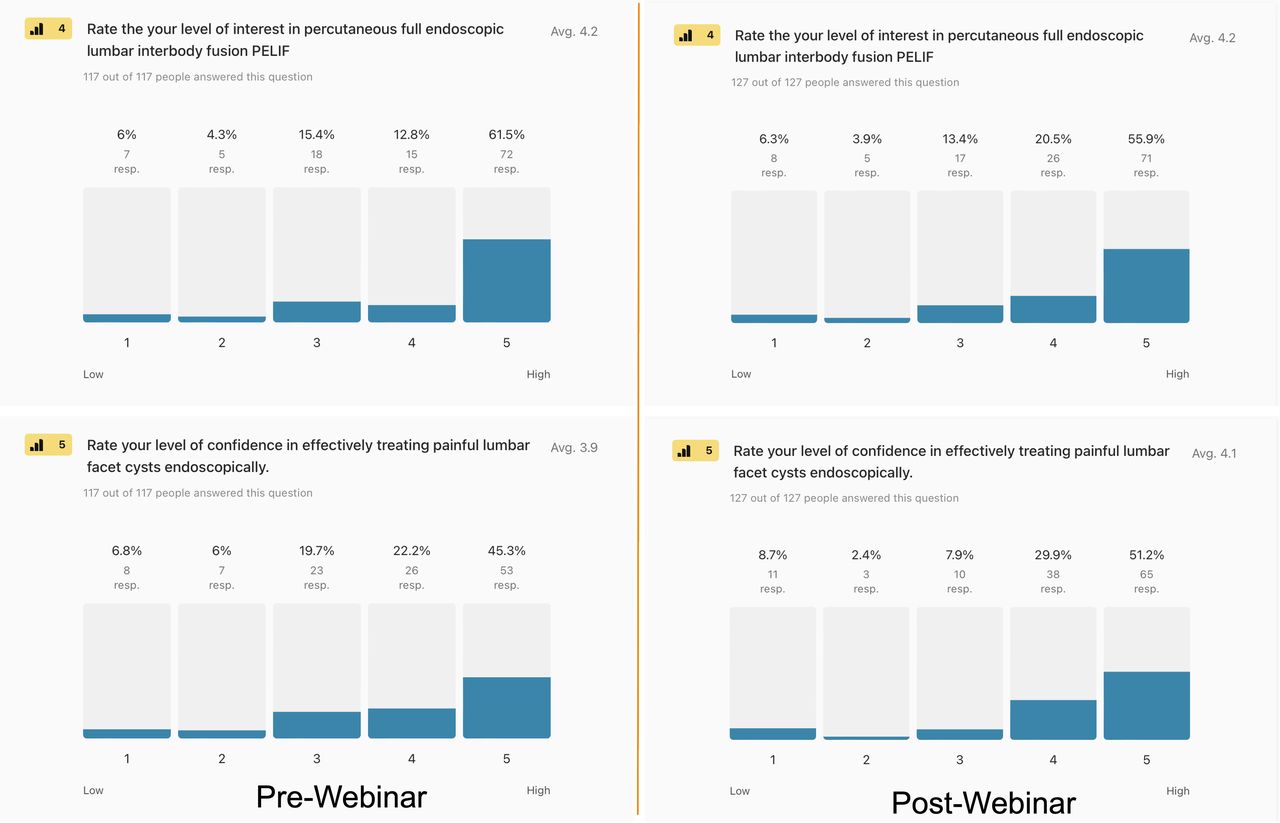
Pre- and postwebinar descriptive statistics of (4) the level of survey respondents’ interest in percutaneous endoscopic lumber interbody fusion (PELIF) at a high level (option 5) was 61.5% and 55.9%, and (5) confidence in effectively treating painful lumbar facet cysts with the endoscopic surgery platform were 45.3% and 51.2%, respectively.

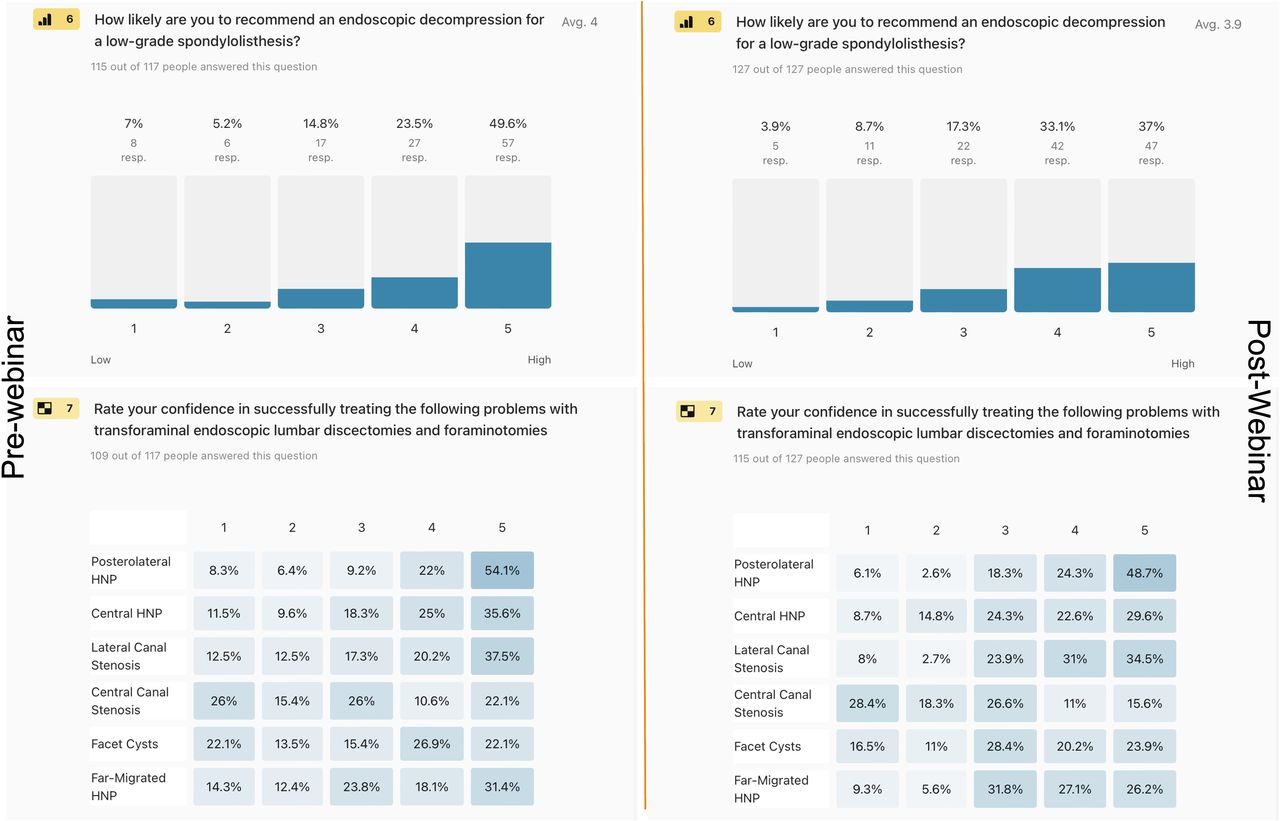
Pre- and postwebinar descriptive statistics as combined percentages of high-level endorsement options 4 and 5 of survey respondents’ (6) likelihood of recommending an endoscopic decompression for spinal stenosis-related symptoms in patients with low-grade lumbar spondylolisthesis (73.4% vs 70.1%), and (7) the confidence in transforaminal endoscopic surgery successfully treating posterolateral herniated disc (76.1% vs 73%), central HNP (60.6% vs 52.2%), lateral canal stenosis (57.7% vs 65.5%), central canal stenosis (32.9% vs 26.6%), facet cysts (49% vs 44.1%), and far-migrated HNP (49.5% vs 53.3%). Abbreviation: HNP, herniated nucleus pulposus.
There was great interest and confidence in procedures that may be considered controversial by traditionally trained spine surgeons, for example, the single-level PELIF with concurrent placement of nonsegmental pedicle screw instrumentation. The interest in PELIF at a high level (option 5) decreased from 61.5% prewebinar to 55.9% postwebinar, as shown in Figure 3. Treatment of lumbar facet cysts with the UBE technique saw an increase in confidence in effectively treating painful lumbar facet cysts using the UBE surgery platform. Confidence in this procedure increased from 45.3% to 51.2% after the webinar, conceivably highlighting a growing trust in this technique (Figure 3). Perhaps the most controversial of all topics presented was the endoscopic decompression of painful degenerative lumbar spondylolisthesis, whose endorsement decreased slightly from 73.4% to 70.1% postwebinar (Figure 3). Nevertheless, nearly three-quarters of respondents considered painful low-grade lumbar degenerative spondylolisthesis an appropriate indication for endoscopic spine surgery. The following varying degrees of confidence changes (Figure 4) occurred from the pre- to postwebinar survey regarding the effectiveness of the transforaminal endoscopic decompression surgery in producing favorable clinical outcomes:
Posterolateral herniated disc: Confidence decreased from 76.1% to 73%.
Central HNP: There was a notable decrease from 60.6% to 52.2%.
Lateral canal stenosis: Confidence increased from 57.7% to 65.5%.
Central Canal stenosis: A decrease was observed from 32.9% to 26.6%.
Facet cysts: Confidence decreased from 49% to 44.1%.
Far-migrated HNP: An increase from 49.5% to 53.3% was noted.
These findings highlighted nuanced shifts in professional opinions and confidence related to various endoscopic spine surgery techniques. Perhaps these shifts indicated the ability of educational interventions to impact surgical practice preferences and perceived efficacy or represented bias or noise in the data. The Rasch methodology was employed to analyze the observed endorsement shifts at a more granular level to filter out those findings that consistently found high surgeon endorsement.
Polytomous Rasch Analysis
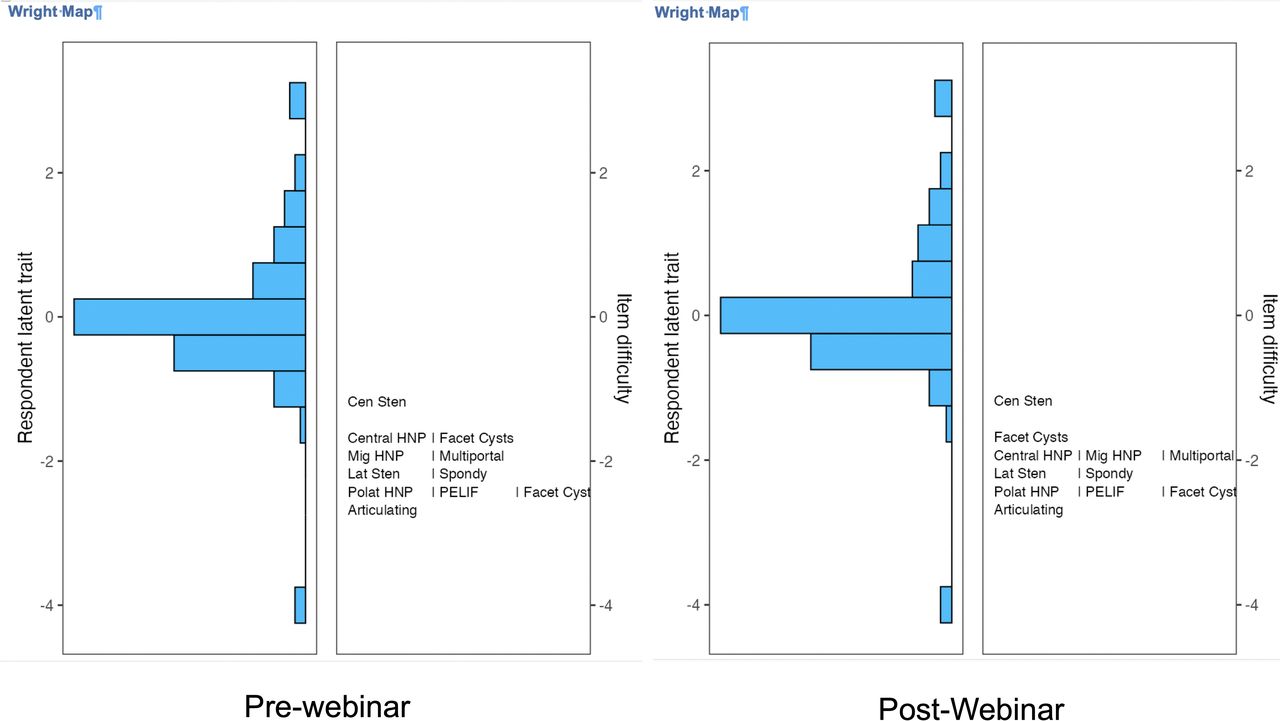
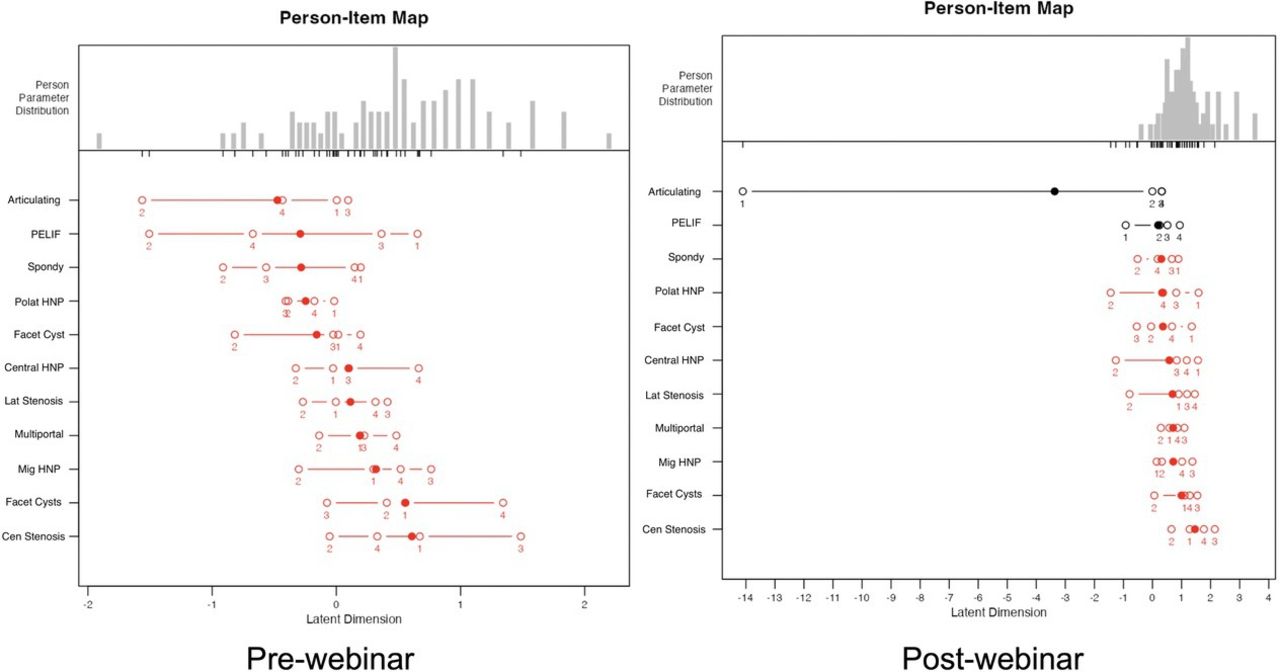
As demonstrated in Figures 5 and 6, the polytomous Rasch analysis offered a nuanced understanding of surgeons’ intensity of endorsements of various procedural techniques. The Wright plots (Figure 5) highlighted a consensus among surgeons on the merit of articulating instruments, transforaminal treatment of posterolateral HNP, PELIF, lateral canal stenosis, and endoscopic decompression of painful low-grade lumbar spondylolisthesis and UBE treatment of symptomatic lumbar facet cysts (Figure 5). The harder-to-agree-on items were transforaminal decompression of facet cysts, migrated HNP, central HNP, and simultaneous use of multiportal techniques mixing transforaminal and translaminar techniques in the same operation. Despite some redundancy between the prewebinar test item lineup, the postwebinar Wright plot was identical. The item hardest to agree on was transforaminal decompression of central HNP.

The item response theory polytomous Rasch partial agreement analysis was employed to obtain Wright plots of prewebinar (left panel) and postwebinar (right panel) survey responses regarding the importance of having articulating instruments, the ability to perform simultaneous uniportal transforaminal and biportal endoscopic surgery, the level of endorsement of percutaneous endoscopic lumbar interbody fusion (PELIF), and endoscopic treatment of low-grade spondylolisthesis (Spondy) lumbar facet joint cysts. In addition, surgeons were asked to rate the confidence in successfully treating central and lateral canal stenosis, central herniated nucleus pulposus (HNP), posterolateral HNP, migrated (Mig) HNP, and facet cysts with the transforaminal approach. On the left side of the Wright plot, the responding surgeons’ latent traits are written in logits (log odds) as estimates of true intervals of item difficulty and surgeon ability and intensity of partial agreement. The surgeons, represented by horizontal bars at the top, represented the highest level of endorsement. On the right of the Wright plot, the harder-to-agree-on items are listed at the top vs the easier-to-agree-on ones at the bottom. Directly across from 0, those surgeons had a 50% chance of endorsing a test item. There were 2 assessment gaps on the prewebinar survey and 1 on the postwebinar survey. The largest gap was created by disagreements on the need for articulating instruments. There was some redundancy between prewebinar test items, as shown by the same ranking for transforaminal treatments of various pathologies. However, endoscopic decompression of central stenosis was considered the hardest. Abbreviations: Can Sten, canal stenosis; Polat, posterolateral.

The person-item map of prewebinar (a) and postwebinar (b) survey responses show the logarithmically transformed person and item positions on a unified continuum using the logit measurement unit, transitioning ordinal data to equal-interval data. This method charts both person and item positions (in logits) along the x-axis. Within Rasch modeling, these values are labeled as “locations” rather than “scores.” A surgeon’s logit location indicates their natural log odds of agreement with a series of items. Individuals with pronounced adherence to the considered attitude affirm items favorably, positioning them further to the right on the scale. The solid dots indicate the mean person location scores. Disordered items are shown in red, and ordered ones are in black. Examining the order and location of these test items reveals an uneven distribution of the ranked order of item difficulties or intensities along the logit continuum, suggesting a poor fit to the Rasch model without any statistically significant difference between the observed values and the values predicted by the model. In comparison to descriptive statistics (Figures 1–3), the most high-intensity items in the prewebinar survey with median log-odds greater than 0 were the pathologies commonly treated with the transforaminal approach, including facet cysts, migrated disc herniations, and lateral and central canal stenosis. The multiportal approach strategy also received a higher than 0 median log odd. Posterolateral disc herniations, percutaneous endoscopic lumbar interbody fusion with endoscopically placed cages and posterior supplemental pedicle screw fixation (PELIF), low-grade spondylolisthesis (Spondy), and the need for articulating instruments during endoscopic treatment of more complex spinal pathologies, and UBE facet joint cyst treatment received log-odds of less than 0 suggesting these items were low intensity. All prewebinar test items had disorderly log odds. The postwebinar analysis showed an endorsement boost for all test items with increased median log odds above 0 except “articulating instruments,” highlighting the high impact of the webinar-based education. However, postwebinar analysis showed orderly item response configuration for articulating instruments and endoscopic treatment of Spondy. Abbreviations: Cen, central; HNP, herniated nucleus pulposus; Lat, lateral; Mig, migrated; Polat, posterolateral; Sten, stenosis.
In comparison to prewebinar descriptive statistics (Figures 1–3), the corresponding prewebinar survey person-item map (Figure 6) revealed that the most high-intensity items were transforaminal treatment of central stenosis, facet cysts, migrated HNP, followed by lateral canal stenosis, and central HNP with all mean logits shifted to the right and being greater than 0; that is, greater than a 50% chance of endorsing the test items. Low-intensity items with logit locations shifted to the left (between 0 and −2) were transforaminal decompression of lumbar facet cysts, posterolateral HNP, spondylolisthesis, PELIF, and articulating instruments. All prewebinar test items revealed disorderly responses on a Likert scale from 1 to 5. The postwebinar person-item map shows a significant endorsement shift with an increase of agreement intensity demonstrated by a shift of the mean logit locations to the right above the +1 logit, suggesting greater than 75% endorsement for central stenosis as the least favorite indication for the transforaminal approach and high-intensity support for and UBE treatment of lumbar facet cysts. The test items transforaminal decompression for central and posterolateral HNP, migrated HNP, lateral canal stenosis, lumbar facet cysts, spondylolisthesis, and PELIF received logit locations between 0 and +1, suggesting 50% to 75% endorsement. The mean logit locations shifted to the right for all test items. Still, they remained out of order, suggesting that some surgeons could not be measured as reliably as the majority by this set of items, indicating the test items were either too intense or not intense enough for them. The only exception was the test item articulating instruments, where the median logit location shifted to the left in the postwebinar survey, suggesting lower endorsement after the webinar for articulating instruments and responding surgeons after the webinar presentation did not consider the latter as relevant. The most significant shift occurred in the test item spondylolisthesis from a disorderly threshold lineup and a median logit location below 0 to an orderly threshold response and a median logit location above 1 (75% endorsement).
Fit and DIF Bias Statistics
Infit and outfit statistics showed that all calculated values were between 0.6 and 1.4 before and after the webinar except for the prewebinar numbers for items transforaminal decompression for posterolateral and central HNP (Table 1); these numbers suggest that both the outlier-sensitive statistics (outfit) and the inlier-sensitive or information-weighted fit statistics, which are more sensitive to the pattern of responses to items targeted on the person, fit the Rasch model well (Tables 1 and 2). The authors also employed the MAPQ3 methodology rooted in IRT analysis with 0.201 (P < 0.001) calculated for the prewebinar survey and 0.180 (P < 0.001) for the postwebinar survey—less than 0.3 corroborating the absence of data distortion. The DIF statistics for the prewebinar survey DIF detection procedure showed no statistically significant difference between orthopedic surgeons (reference group) and neurosurgeons (focal group; Table 3) in item response characteristics curves shown in Figures 7–12. However, the DIF statistics for the postwebinar survey DIF detection procedure showed a statistically significant difference between orthopedic surgeons (reference group) and neurosurgeons (focal group; Table 4), regarding the items articulating instruments and PELIF, therefore indicating data distortion suggestive of bias for these test item in the postwebinar survey (Table 4, Figures 11 and 12).
Prewebinar survey model fit analysis and item statistics of the rating scale model.
Postwebinar survey model fit analysis and item statistics of the rating scale model.
Prewebinar survey DIF detection procedure for ordinal data based on adjacent category logit model.

Item characteristic curves generated from prewebinar survey responses to multiportal treatment for complex lumbar spinal pathologies as part of a differential item functioning (DIF) detection process to detect item bias between orthopedic surgeons and neurosurgeons using the difNLR() and difORD() functions. Specifically, when DIF is identified in an item, 2 distinct curves are generated: 1 for the reference group (orthopedic surgeons) and another for the focal group (neurosurgeons). Alongside these curves, empirical probabilities are visualized as points, which indicate the proportion of correct responses relative to the participant’s ability level and group. The size of these points reflects the number of respondents at each ability level which showed no significant difference between orthopedic surgeons (reference group) and neurosurgeons (focal group) with the statistics for prewebinar DIF detection of 0.0236 and a P value of 0.878 (Table 3) compared with postwebinar DIF detection of 1.607 and a P value of 0.448 (Table 4). There were no discernable differences between orthopedic surgeons and neurosurgeons.

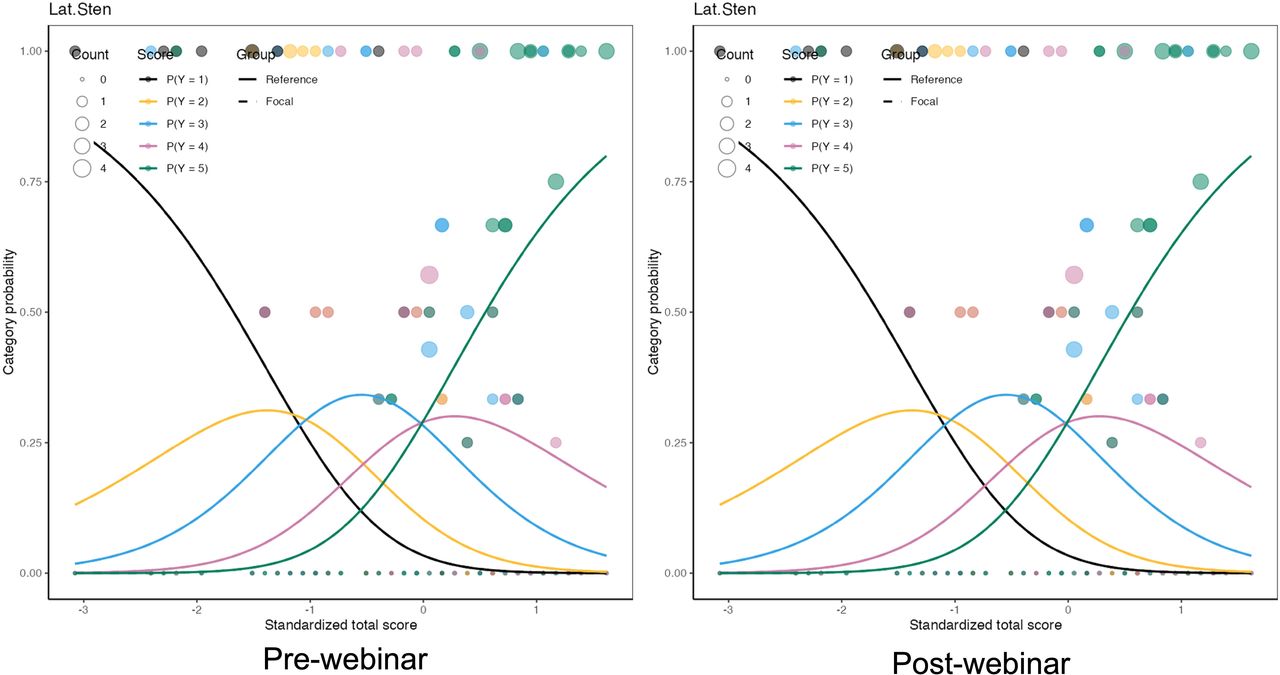
Item characteristic curves generated from prewebinar survey responses “Lateral Canal Stenosis” (Lat. Sten.) as part of a differential item functioning (DIF) detection process to detect item bias between orthopedic surgeons and neurosurgeons using the difNLR() and difORD() functions. Specifically, when DIF is identified in an item, 2 distinct curves are generated: 1 for the reference group (orthopedic surgeons) and another for the focal group (neurosurgeons). Alongside these curves, empirical probabilities are visualized as points, which indicate the proportion of correct responses relative to the participant’s ability level and group. The size of these points reflects the number of respondents at each ability level which showed no significant difference between orthopedic surgeons (reference group) and neurosurgeons (focal group) with the statistics for prewebinar DIF detection of 0.3394 and a P value of 0.560 (Table 3) compared with postwebinar DIF detection of 0.198 and a P value of 0.906 (Table 4). There were no discernable differences between orthopedic surgeons and neurosurgeons.

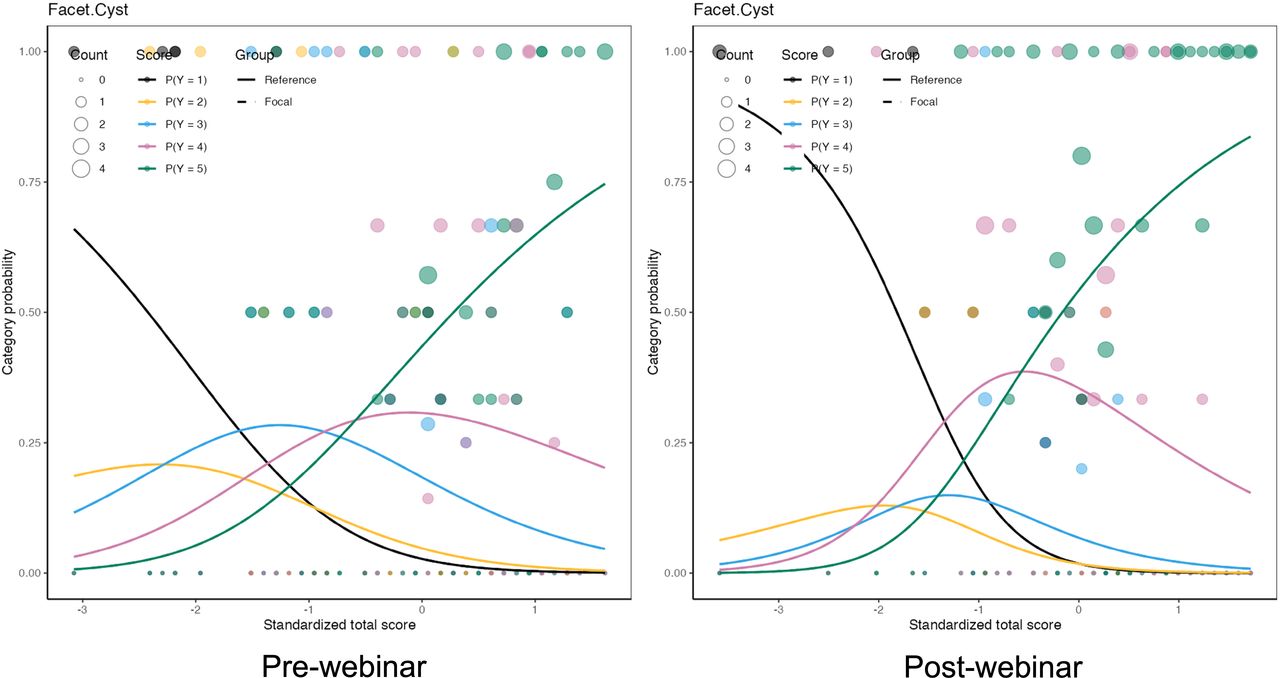
Item characteristic curves generated from prewebinar survey responses unilateral biportal endoscopic facet cyst as part of a differential item functioning (DIF) detection process to detect item bias between orthopedic surgeons and neurosurgeons using the difNLR() and difORD() functions. Specifically, when DIF is identified in an item, 2 distinct curves are generated: 1 for the reference group (orthopedic surgeons) and another for the focal group (neurosurgeons). Alongside these curves, empirical probabilities are visualized as points, which indicate the proportion of correct responses relative to the participant’s ability level and group. The size of these points reflects the number of respondents at each ability level which showed no significant difference between orthopedic surgeons (reference group) and neurosurgeons (focal group) with the statistics for prewebinar DIF detection of 0.8608 and a P value of 0.354 (Table 3) compared with postwebinar DIF detection of 1.284 and a P value of 0.526 (Table 4). There were no discernable differences between orthopedic surgeons and neurosurgeons.

Item characteristic curves generated from prewebinar survey responses regarding Spondy (low grade spondylolisthesis) as part of a differential item functioning (DIF) detection process to detect item bias between orthopedic surgeons and neurosurgeons using the difNLR() and difORD() functions. Specifically, when DIF is identified in an item, 2 distinct curves are generated: 1 for the reference group (orthopedic surgeons) and another for the focal group (neurosurgeons). Alongside these curves, empirical probabilities are visualized as points, which indicate the proportion of correct responses relative to the participant’s ability level and group. The size of these points reflects the number of respondents at each ability level which showed no significant difference between orthopedic surgeons (reference group) and neurosurgeons (focal group) with the statistics for prewebinar DIF detection of 0.6184 and a P value of 0.432 (Table 3) compared with postwebinar DIF detection of 8.130 and a P value of 0.017 (Table 4). There were no discernable differences between orthopedic surgeons and neurosurgeons.

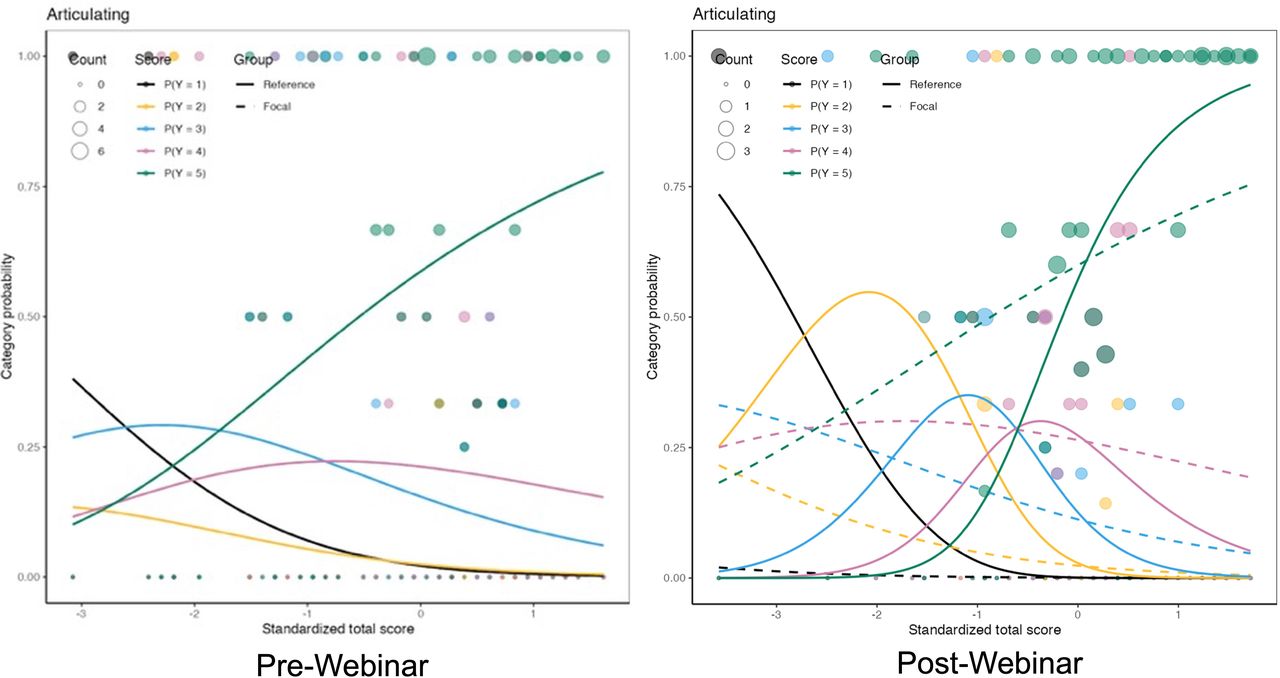
The item characteristic curves generated from prewebinar survey responses regarding articulating instruments as part of a differential item functioning (DIF) detection process to detect item bias between orthopedic surgeons and neurosurgeons using the difNLR() and difORD() functions. Specifically, when DIF is identified in an item, 2 distinct curves are generated: 1 for the reference group (orthopedic surgeons) and another for the focal group (neurosurgeons). Alongside these curves, empirical probabilities are visualized as points, which indicate the proportion of correct responses relative to the participant’s ability level and group. The size of these points reflects the number of respondents at each ability level which showed significant difference between orthopedic surgeons (reference group) and neurosurgeons (focal group) with the statistics for prewebinar DIF detection of 0.5462 and a P value of 0.460 (Table 3) compared with postwebinar DIF detection of 11.168 and a P value of 0.004 (Table 4), suggesting significant bias in the merit assessment of “Articulating Instruments” between orthopedic surgeons and neurosurgeons with disorderly responses in the item’s midsection while maintaining good discriminatory fusion between low- and high-level endorsement.

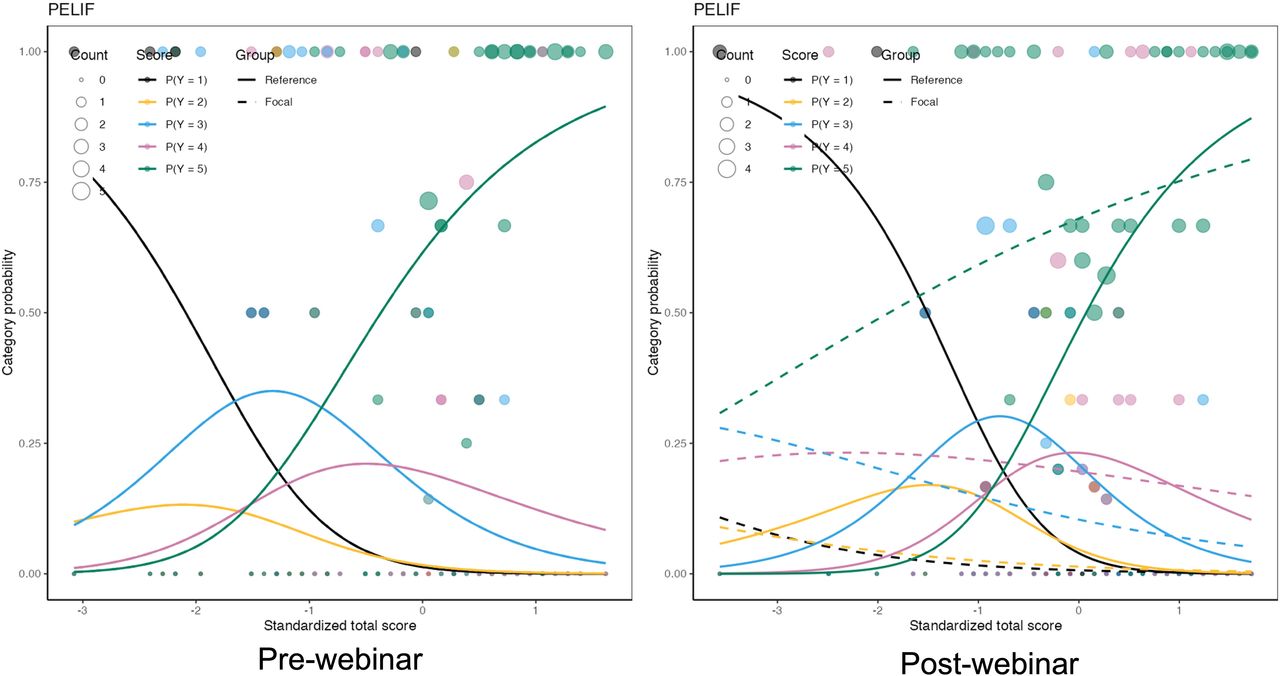
The item characteristic curves generated from prewebinar survey responses regarding percutaneous endoscopic lumbar interbody fusion (PELIF) as part of a differential item functioning (DIF) detection process to detect item bias between orthopedic surgeons and neurosurgeons using the difNLR() and difORD() functions. Specifically, when DIF is identified in an item, 2 distinct curves are generated: 1 for the reference group (orthopedic surgeons) and another for the focal group (neurosurgeons). Alongside these curves, empirical probabilities are visualized as points, which indicate the proportion of correct responses relative to the participant’s ability level and group. The size of these points reflects the number of respondents at each ability level which showed significant difference between orthopedic surgeons (reference group) and neurosurgeons (focal group) with the statistics for prewebinar DIF detection of 0.8548 and a P value of 0.355 (Table 3) compared with postwebinar DIF detection of 15.485 and a P value of <0.001 (Table 4), suggesting significant bias in the merit assessment of PELIF between orthopedic surgeons and neurosurgeons with disorderly responses in the item’s midsection while maintaining a good discriminatory function between high and low endorsement.
Postwebinar survey DIF detection procedure for ordinal data based on adjacent category logit model.
Discussion
The webinar series on “Current And Emerging Techniques In Endoscopic Spine Surgery” hosted by the ISASS underscores the growing interest and current practice trends in endoscopic spine surgery. The third webinar out of a series 4 has significantly influenced the perceptions regarding PELIF with supplemental pedicle screw fixation, endoscopic treatment of low-grade spondylolisthesis, multiportal strategies with use of articulating instruments, the UBE treatment of painful lumbar facet cysts, and suitability of the transforaminal approach to treat common painful degenerative conditions of the lumbar spine ranging from posterolateral, migrated, and central HNP, central and lateral canal stenosis. With significant online attendance and active participation in pre- and postwebinar surveys, the survey completion rates were high with 77.3% prewebinar and 75.7% postwebinar, reflecting an effective surgeon engagement. The representation across different specialties and experience levels suggests a broad-based interest in endoscopic spine surgery techniques, with a predominance of orthopedic surgeons over neurosurgeons.
Descriptive Opinion Statistics
There are nuanced shifts in surgeons’ perceptions and confidence regarding various procedural applications. These shifts highlight the potential influence of educational interventions on shaping clinical practice and the understanding of complex surgical techniques. The slight increase in the endorsement of articulating instruments for complex endoscopic decompressions—from 79.4% before the webinar to 81.4% afterward—suggests a growing appreciation for these tools’ utility in facilitating complex procedures. This change, although modest, may reflect an enhanced recognition of the technical advantages these instruments provide during surgery, as discussed during the webinar. Conversely, the slight decline in the perceived benefits of multiportal technique flexibility, from 62.4% to 58.2%, could indicate a reassessment of this approach’s practicality or perhaps just variability in the data. It is possible that further discussion and demonstration of these techniques could either solidify their perceived utility or confirm a trend toward preferring traditional methods.
Notably, changes in attitudes were also observed toward more controversial procedures such as PELIF and the treatment of lumbar facet cysts using the UBE technique. The decrease in high-level interest in PELIF, alongside an increase in confidence in treating lumbar facet cysts with the UBE technique, points to a dynamic shift in trust and skepticism among the endoscopic spine surgeons. These changes may represent a reevaluation of the risks and benefits associated with each procedure, influenced by the latest clinical evidence and peer discussions presented during the webinar. Further variations in confidence were noted across different conditions treated with transforaminal endoscopic decompression surgery. Decreases in confidence for treating conditions like central HNP and central canal stenosis were paralleled by increases in treating lateral canal stenosis and far-migrated HNP. These contrasting trends could be indicative of the evolving understanding of where endoscopic techniques may be most effectively applied, as influenced by the detailed procedural insights provided during the webinar.
The most intriguing observations arose from the pre- to postwebinar assessments of the endorsement for endoscopic decompression of painful degenerative lumbar spondylolisthesis, where nearly three-quarters of the respondents considered it a viable option postwebinar, despite a slight decrease in endorsement. This strong ongoing support might reflect a solid baseline belief in the efficacy of endoscopic techniques for this condition, moderated slightly by the detailed discussions of potential challenges and limitations shared during the webinar.
Rasch Survey Analysis
The Rasch analysis methodology provided a deeper understanding of these shifts by examining the consistency of high endorsements across different surgical techniques. This analysis helped distinguish between genuine shifts in clinical opinion and variations that might represent statistical noise or bias in the survey responses. Most of the survey questions (items) categories did discriminate well, and the observed data did follow the predictions by the Rasch model well, with most of the outfits just around 1, except test items transforaminal posterolateral HNP and transforaminal central HNP. Outfit statistics of less than 1 would suggest that the data are less variable than the Rasch model expects—they would have been over-predictable (Tables 1 and 2). These observations for test items PELIF, transforaminal facet cyst treatment, low-grade spondylolisthesis, transforaminal central stenosis, and multiportal technique could indicate redundancy among items (eg, questions that were too similar to each other) or that some items are not contributing useful information for distinguishing among respondents. Essentially, it could imply that some survey questions were too easy and did not add value to the measurement process. While values close to 1.0 are ideal, a range of 0.7 to 1.3 typically indicates a good fit. However, very low outfit values were not observed. If so, they would generally be less concerning than high values, as they do not indicate noise caused by outliers. The observed infit and outfit values suggested that the authors’ survey instrument questions displayed good efficiency except for the prewebinar test items transforaminal posterolateral HNP, transforaminal central HNP, and multiportal technique, where the outfit values were high, 1.576 and 1.752, respectively.
The authors also learned from the pre- and postwebinar Wright plots that the transforaminal endoscopic surgery for central stenosis, central and migrated HNP, facet cysts, and multiportal techniques generated high-intensity responses and were the hardest to agree on (Figure 4). Transforaminal surgery for posterolateral HNP and low-grade spondylolisthesis was much easier to agree on. These observations are corroborated by multiple clinical studies illustrating the effectiveness of the transforaminal technique in these applications.14–19 The UBE technique to treat lumbar facet joint cysts, the PELIF, and articulating instruments was agreed on as the easiest and endorsed for these indications.
The person-item maps revealed disordered threshold responses for all test items in the prewebinar survey (Figure 5). This pattern typically results from category overlap or reversal, suggesting that participants may have struggled to differentiate between certain levels of agreement or endorsement. Such disordered responses, exhibiting intense polarization between agreement and disagreement, often arise when the sequence of response categories fails to show a clear, linear progression. This confusion can stem from ambiguity in the response categories or the item’s complexity, causing varied interpretations among respondents. Another contributing factor could be the response scale’s lack of sensitivity in capturing subtle distinctions in attitudes or perceptions, which might lead to unexpected reversals in category usage. Practically, these disordered responses highlight the need for further scrutiny to refine survey questions and adjust the response scale to enhance clarity and resolve the issues with disordered items. However, the authors could not perform a calibration or refinement to reduce redundant or overly predictable items since there were no “right” or “wrong” external criteria. They used the Rasch methodology to examine the incoming survey data. They carefully arrived at their consensus interpretation by concentrating on endorsement shifts with an orderly threshold lineup. Surprisingly, such an orderly and strong endorsement shift was observed for the transforaminal decompression of painful low-grade lumbar spondylolisthesis. This finding has also been reported in recent peer-reviewed and published literature.20–23
Limitations and Bias Detection
High item complexity and lack of scale sensitivity may have been relevant limitations of our Rasch analysis. As discussed in more detail in the article on the second ISASS webinar on contemporary endoscopic spinal surgery techniques, the authors employed the difORD() functions for bias detection rather than traditional analysis of variance and regression analysis which may be flawed if they are based on an external criterion that relies on the assumption that the criterion is an unbiased measure. The difficulty of constructing an unbiased criterion calls for using only an internal criterion, and hence, only the information contained in the responses of persons to test items. The Rasch logistic response model can overcome this limitation by using internal criteria to evaluate and measure responses to items within a test or survey. The maximum likelihood estimation techniques applicable to the Rasch model lead to useful asymptotic estimates of the variance of parameter estimates. All this makes it possible to identify tests that are biased in ways that do not change the relative difficulties of items but rather their scale of measurement, to separate biased items from items that misfit for other reasons, and to specify the magnitude of residual variance to be expected when items and persons together fit the measurement model. Therefore, the authors’ observations regarding surgeon responses can be considered a largely unbiased representation of current trends (Figures 6–9) except for the items articulating instruments and PELIF, where the DIF statistics for the postwebinar survey DIF detection procedure showed a statistically significant difference between orthopedic surgeons (reference group) and neurosurgeons (focal group), thus clearly indicating data distortion suggestive of bias for these test 2 items in the postwebinar survey (Table 4, Figures 10 and 11).
Conclusions
The findings in the third ISASS webinar on Contemporary Endoscopic Spinal Surgery Techniques underscore the significant impact of targeted educational programs on surgical practices, potentially driving future clinical guidelines and training programs to better align with evolving techniques and surgeon confidence levels. The continued evaluation of these educational interventions is essential to ensure they effectively address the needs and uncertainties of innovator surgeons attempting to promote best practices in endoscopic spine surgery. The polytomous Rasch analysis of partial procedural endorsements illustrated the ongoing dynamic shifts in preferences and consensus on best practices in endoscopic spine care regarding treatment advances in patients with low-grade spondylolisthesis and those needing fusion. The key takeaways from the third webinar’s surveys and analyses underscore the high acceptance of transforaminal decompression for posterolateral disc herniations and lateral canal stenosis and the UBE technique for endoscopic treatment of painful lumbar facet cysts.
Acknowledgments
This webinar and special issue were supported with an education grant to ISASS from Lange MedTech.
Footnotes
↵† International Society for the Advancement of Spine Surgery, Interamerican Society for Minimally Invasive Spine Surgery - La Sociedad Interamericana de Cirugía de Columna Mínimamente Invasiva (SICCMI), International Intradiscal Therapy Society
↵‡ Interamerican Society for Minimally Invasive Spine Surgery - La Sociedad Interamericana de Cirugía de Columna Mínimamente Invasiva (SICCMI)
↵§ International Society for the Advancement of Spine Surgery
Funding ISASS received funding for the webinar series upon which this article is based as well as for the publication of this special issue. Funding was paid directly to ISASS. No formal funding by private, government, or commercial funders was received by the authors.
Declaration of Conflicting Interests The authors volunteered their time and internal resources to support the design and conduction of this research study. All authors aided in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results. The authors declare no conflict of interest relevant to this research, and there was no personal circumstance or interest that may be perceived as inappropriately influencing the representation or interpretation of reported research results. This research was not compiled to enrich anyone.
Disclosures Brian Kwon reports royalties for product design from Globus/NUVA; consulting fees from Globus/NUVA for evaluation of products and technology; payment/honoraria for surgeon education/training from Globus/NUVA and Amplify Surgical; and stock/stock options in Amplify Surgical and SAB. Choll Kim reports consulting fees from Elliquence and Globus Medical.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.