


Abstract
Background Unilateral biportal endoscopy (UBE) is a minimally invasive approach to treat cervical spondylotic radiculopathy (CSR), which is a common condition caused secondary to disc herniation, disc degeneration, uncal osteophytes, and other conditions manifesting as neuropathic radicular pain. Anterior cervical discectomy and fusion (ACDF) is the gold standard surgical technique for treating CSR. However, it has several disadvantages, including loss of mobile segment, adjacent segment degeneration (ASD), implant- and approach-related complications, and high hospitalization costs.
Objective The current study aimed to evaluate the safety and efficacy of UBE decompression for CSR.
Methods After obtaining IRB approval, a single-center retrospective study was undertaken. Included patients underwent UBE decompression for CSR with a minimum of 6 months of follow-up. Patient demographics, perioperative data, and length of hospital stay were reviewed. Clinical outcomes were assessed using VAS scores for neck and arm pain, and NDI scores were measure preoperatively and at 1 and 6 months after UBE decompression. A repeated analysis of variance test was performed to measure the difference between VAS and NDI scores.
Results Twenty patients (M: 15, F: 5) with a mean age of 56.7 ± 10.2 years were included. The mean follow-up period was 8.4 ± 1.8 months. The mean surgical time was 64.3±10.6 minutes. The average length of hospital stay was 1 day. At the final follow-up, the mean VAS for arm pain improved from 6.4 ± 0.7 to 0.6 ± 0.5 (92% improvement) and the mean VAS for neck pain improved from 3.3 ± 0.4 to 2.0 ± 0.2 (40% improvement). NDI score improved from 23.2 ± 1.95 to 5.7 ± 0.6 at the final follow-up (75% improvement). There were no complications.
Conclusion UBE is a safe and effective surgical treatment option for patients with CSR with excellent clinical outcomes.
Clinical Relevance Clinical relevance of this case series study is to demonstrate the safety and efficacy of the novel unilateral biportal endoscopic decompression of cervical spondylotic radiculopathy and its short term clinical outcomes.
Level of Evidence 4.
Introduction
Cervical spondylotic radiculopathy (CSR) is a common degenerative spinal disease with an increasing prevalence. CSR may be caused by nerve root compression from disc degeneration, herniation, segmental instability, or other disorders, resulting in neuropathic radicular pain.1 Most CSR patients respond well with conservative management in the form of medications and physiotherapy.2 Surgery is reserved for patients who are refractory to conservative management or who have neurological deterioration. Anterior cervical discectomy and fusion (ACDF) has been considered a gold standard surgical treatment option for the management of CSR.3,4 However, it is associated with increased risk of adjacent segment disease, loss of motion, implant-related complications, nonunion, increased length of hospital stay, and cost.5–8 In addition, the anterior approach to the cervical spine is associated with an increased risk of postoperative dysphagia,9,10 esophageal perforation,11 and iatrogenic injury to major neurovascular structures.12 Cervical disc replacement emerged as a novel technique to address certain issues associated with ACDF.13 However, it has its limitations of subsidence, expulsion, heterotrophic ossification, persistent neck pain, increased cost, and approach-related complications.14
The other option to treat CSR is posterior cervical foraminotomy. It addresses the issues associated with anterior surgery; however, it has its drawbacks in the form of axial neck pain, inadequate decompression, operative bleeding, paraspinal muscle spasm, and loss of normal alignment after surgery.15,16 Recently, the percutaneous endoscopic foraminotomy technique emerged as a safe minimally invasive surgical treatment option to conventional microsurgical techniques.17 Unilateral biportal endoscopy (UBE) is a newer endoscopic technique that uses 2 portals (scope portal and working portal) on the same side of the spine to provide excellent magnification and visualization of the spinal structures.18 There is a paucity of literature on the application of the UBE cervical foraminotomy technique for CSR patients. The current study sought to evaluate the short-term clinical outcomes of the UBE decompression technique for CSR patients by a single surgeon.
Materials and Methods
After obtaining Institutional Review Board approval, we performed a single-center retrospective study and included patients who underwent UBE for CSR from April 2023 to May 2024 with a minimum of 6 months of follow-up. A total of 25 patients underwent UBE for CSR during this period. The inclusion criteria were as follows: (1) Patients with cervical radicular symptoms without severe neck pain and refractory to conservative management for at least 6 to 8 weeks; (2) a diagnosis of CSR based on clinical history, physical examination, and imaging studies; (3) single-level pathology; (4) absence of central pathology causing myelopathy; (5) the absence of significant instability, infection, fracture, or previous spinal surgery history; and (6) minimum of 6 months of follow up. Patients with cervical spondylodiscitis, cervical myelopathy due to ossification of the posterior longitudinal ligament, or cervical spine trauma were excluded. Five patients were excluded due to shorter follow-up; thus, 20 patients were included in the study. Patient’s demographic data, perioperative data, and length of hospital stay were reviewed. Clinical outcomes were assessed using visual analog scale (VAS)19 scores for neck and arm pain and Neck Disability Index (NDI)20 preoperatively and at 1 and 6 months. Written informed consent was obtained from the patient and their family.
Surgical Technique
Patient Position
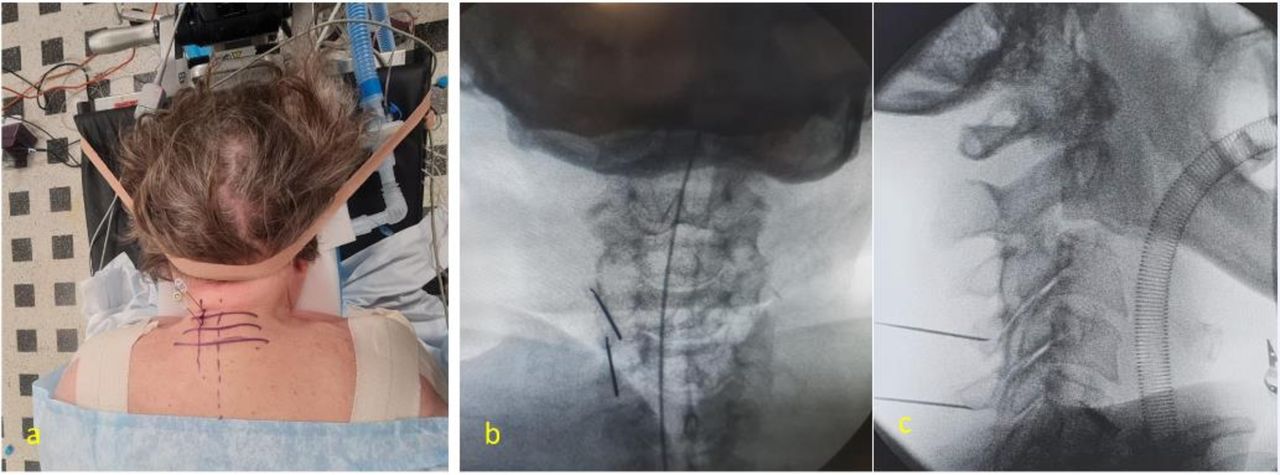
Under general anesthesia, the patient is positioned prone on a radiolucent table. Eyes and chin are protected from direct pressure using foam blocks, and the neck is slightly flexed and fixed with plaster tapes. Traction is applied on the shoulders bilaterally and fixed with plaster tapes as well. The abdomen is relaxed using an H-shaped pillow to avoid increased abdominal pressure. A head-end-up, feet-end-down slanted position is applied to ensure good venous return to reduce chances of intraoperative bleeding (Figure 1).

Patient prone on Jackson table with Gillespie pillow support to reduce abdominal pressure.
Level Marking and Incisions
After proper positioning of the patient, the surgical level is marked under fluoroscopic guidance in both anteroposterior (AP) and lateral projection. Sometimes it becomes difficult to localize the C6 to C7 and C7 to T1 level under lateral fluoroscopy view due to overlapping soft tissues of the shoulders; thus, a proper AP view is necessary. To mark 2 portals, two 18-gauge spinal needles are placed on the cranial and caudal midpoint of the lateral mass of the target level under the guidance of true AP and lateral fluoroscopy projection (Figure 2). The distance between the 2 portals is normally kept around 2 cm to avoid crossinterference. We inject around 0.5 mL methylene blue dye through the spinal needles to help in identifying the level intraoperatively as the dye stains the area. Alternatively, a check c-arm fluoroscopic image can be taken with an instrument inside to confirm the level. Next step is to make the incisions for the portals. In our practice, we make the camera portal incision first, and then, we proceed to make the incision on the working portal. The cervical fascia must be incised with a size 10 blade to ensure proper functioning of portals and also for adequate drainage of irrigation fluid. At our center, we use 3000 cc saline bag and placed it at a height of around 40 cm above the operation area and adjust as per the flow. This height normally keeps flow pressure below 30 mm Hg and avoids damage to the cord. Serial dilators are inserted to dissect the neck muscle and acquire operative space around the V-point (junction of superior and inferior lamina with the medial point of facet joint). Triangulation is done with a 0° scope inserted through the scope portal and a surgical instrument through the working portal.

(a) Showing two 18 gauge spinal needles inserted on midpoint of C4 and C5 lateral masses. (b and c) Showing AP and lateral fluoroscopic images, respectively, of needle placement.
Foraminotomy and Decompression
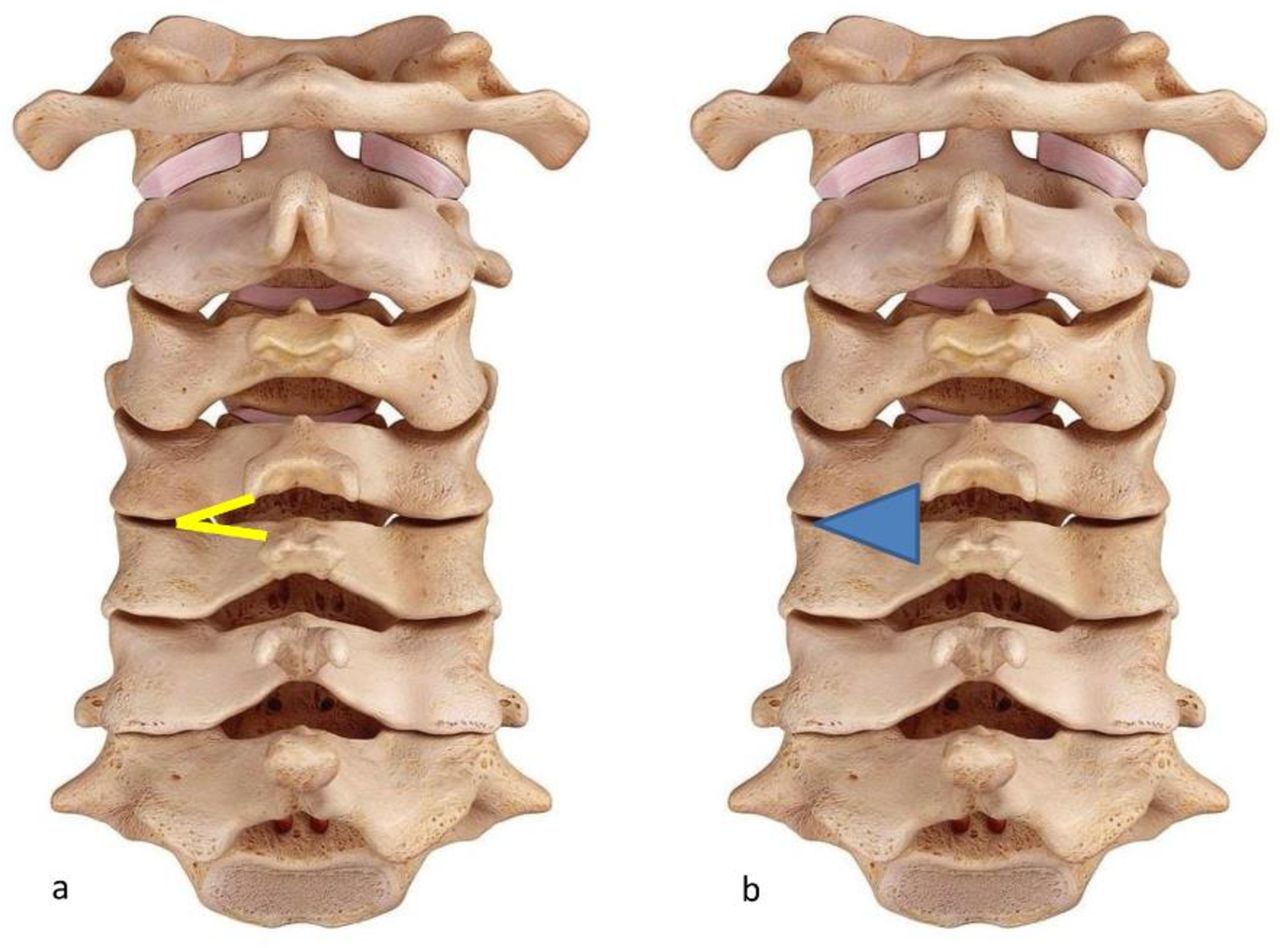
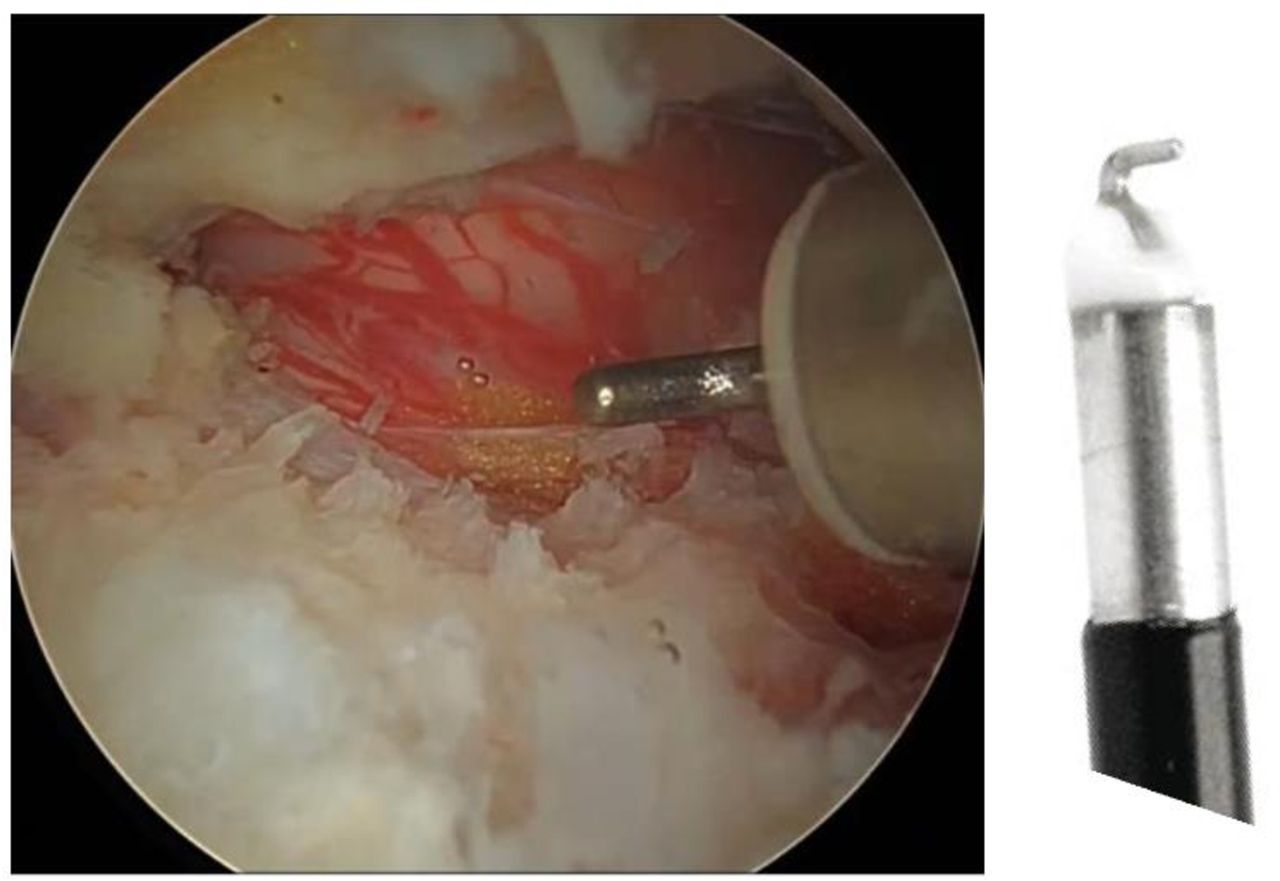
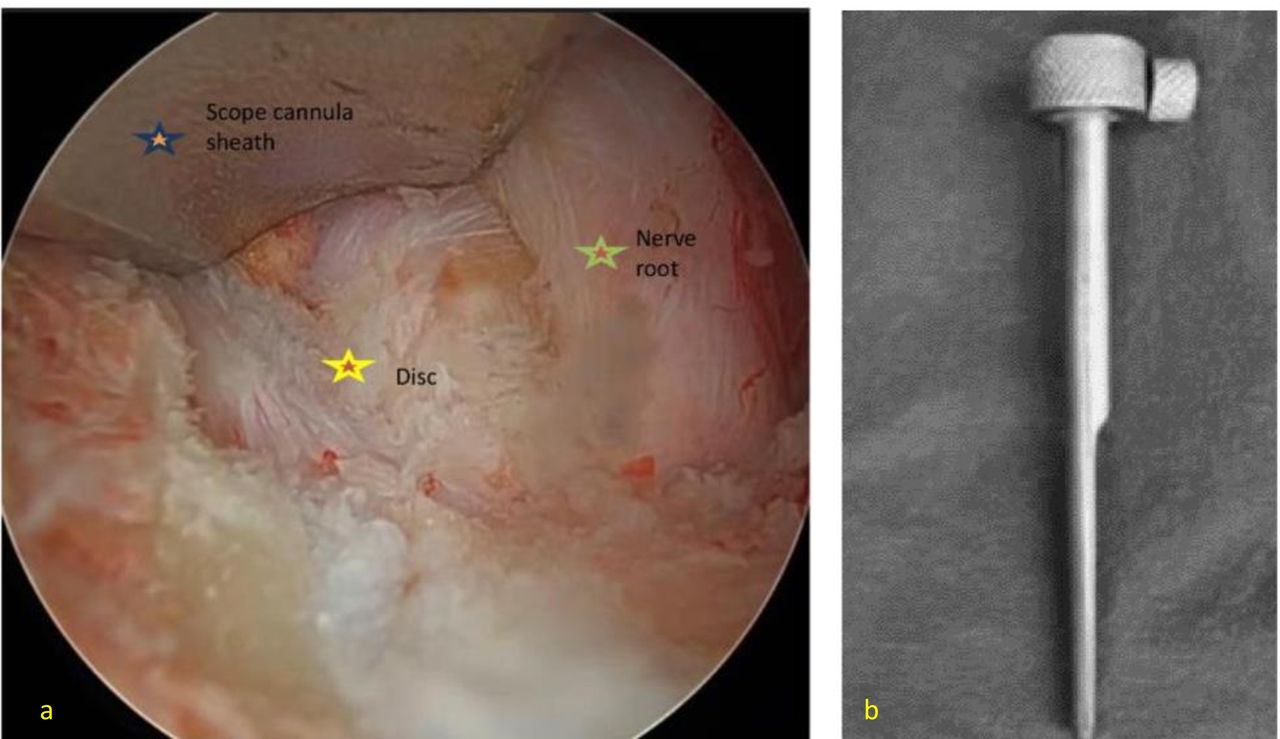
With the radiofrequency probe, soft tissues around the V-point are cleared, bleeding is controled, and the surgical field is exposed. Partial laminectomy-facetectomy is done using a 3.5-mm diamond tip burr starting from the V-point (Figure 3). The inferolateral portion of the cranial lamina is drilled in a craniolateral direction until the attachment of ligament flavum. Similarly, the superolateral portion of the caudal lamina is drilled in a caudolateral direction until the bone is thin like an eggshell. Following this, the medial one-third to one-half is progressively removed. Up to 50% of the facet joint can be removed without causing iatrogenic instability.21,22 The ligamentum flavum is preserved until the bone work is done to prevent accidental injury to the neural structures while drilling. Once the flavum is removed, the medial border of the pedicle is identified first to establish the surgical anatomy of the dura and the nerve root. At this stage, we normally used hook-tipped radiofrequency probe to achieve hemostasis safely (Figure 4). The exiting nerve root is identified and decompressed with a 1-mm Kerrison punch. If the pathology is a disc herniation, the nerve root is safely retracted using the scope cannula sheath (Figure 5), and the disc herniation is safely removed. If there is less workspace to remove the disc, pediculotomy can be done to achieve more space around the nerve root so that it can be retracted safely. Using a ball tip hook, the lateral margin of the pedicle is palpated to ensure adequate foraminal decompression. Irrigation flow is stopped, and a hemostatic agent (Floseal- Baxter) is injected through the working portal and kept for 2 minutes before flushing out. The Floseal consists of a bovine-derived gelatin component and a human-derived thrombin component mixed with prefilled sodium chloride solution. The patient is checked again for any bleeders before closure. We normally do not put in a drain. Closure is done with subcutaneous suture with monocry-l and steristrips applied over it.

(a) V-point which is the junction of superior and inferior lamina with the medial aspect of facet joint. (b) Area marked is the extent of partial laminectomy-facetectomy.

Hook-tipped radiofrequency probe to coagulate epidural vessels.

(a) Scope cannula sheath safely retracting nerve root to expose the disc. (b) Scope cannula sheath.
Illustrated Case 1: C6 to C7 Left Discectomy
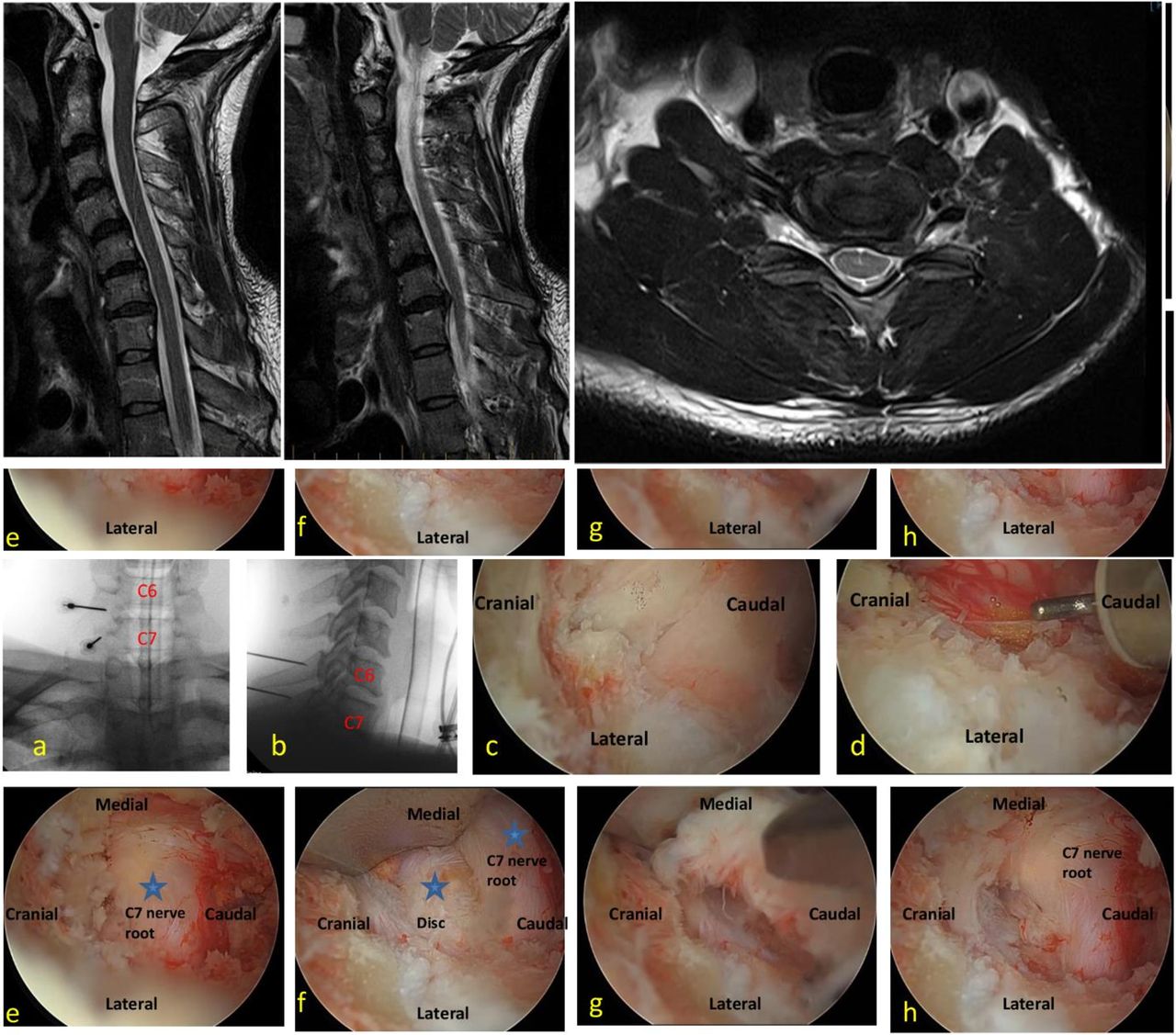
A 37-year-old man came to our outpatient clinic with neck pain radiating to the left upper limb and pins and needles for 8 weeks. Neck pain had a VAS score of 3, while upper limb pain had a score of 7. Examination results showed a positive Spurling sign, a Medical Research Council grade 4 for triceps, and hypoesthesia in the left C7 dermatome. Conservative care, which included medication, rest, and physical therapy, did not work. An MRI revealed that the C7 nerve root was compressed by a left C6 to C7 paracentral disc herniation (Figure 6). V-point and the left C6 to C7 interlaminar space were identified. The underlying flavum was exposed with a partial hemilaminectomy and facetectomy of C6 to C7. The ligamentum flavum was removed, and the C7 nerve root was retracted gently using a scope cannula sheath to expose the bulging disc. Prolapsed disc fragment was removed, and C7 nerve root was decompressed (Figure 6). On the first postoperative day, the VAS was 3 for neck pain and 1 for pain in the left upper limb. Three weeks after surgery, C7 motor function was back to normal.

T2-weighted magnetic resonance images with sagittal, left oblique, and axial views showing C6–C7 left-sided paracentral disc herniation compressing the left C7 nerve root. (a and b) Spinal needle placement and level marking. (c) Identifying the V point and drilling the C6 inferior lamina and C7 superior lamina along with C6–C7 facet joint till the bone is like an eggshell. (d) The ligamentum flavum is exposed and epidural vessels coagulated with a hook-tipped radiofrequency probe. (e) The C7 nerve root is exposed. (f) Scope cannula sheath retracting the C7 nerve root to expose the disc. (g and h) Disc fragment removed and C7 nerve root decompressed.
Statistical Analysis
Data were presented as mean ± SD or SEM. Data analysis was done using SPSS version 13. Repeated analysis of variance test was used to assess statistical significance. P value < 0.05 was considered statistically significant.
Results
The cohort consisted of 20 patients. The demographic parameters are shown in Table 1. The mean follow-up period was 8.4 ± 1.8 months (7–11 months). The pathology causing cervical nerve root compression is summarized in Table 2. The mean length of hospital stay was 1 day. The mean duration of surgery was 64.3 ± 10.6 minutes (Table 3). Exact estimated blood loss could not be recorded due to continuous water irrigation throughout the procedure. The majority of the patients were ambulatory within 24 hours. No immediate or delayed complications were recorded.
Demographic data of patients (n = 20) undergoing unilateral biportal endoscopic decompression for cervical spondylotic radiculopathy.
Pathology causing cervical nerve root compression.
Operative and perioperative data.
Clinical outcome measures are listed in Table 4. At the final follow-up, the mean VAS for arm pain improved from 6.4 ± 0.7 to 0.6 ± 0.5 (92% improvement), and the mean VAS for neck pain improved from 3.3 ± 0.4 to 2.0 ± 0.2 (40% improvement). NDI score significantly improved from 23.2 ± 1.95 to 5.7 ± 0.6 (75% improvement).
Clinical outcome measures: VAS score for arm and neck pain and NDI score.
Discussion
CSR is 1 of the most commonly seen conditions in an outpatient spine clinic. Most patients experience neuropathic radicular pain, which is typically managed conservatively. However, if conservative treatment fails, surgical decompression is recommended to alleviate symptoms. The most important aspect of CSR surgical therapy is the effective decompression and release of nerve structures. This can be accomplished by a variety of surgical procedures, including ACDF, cervical disc replacement, conventional posterior foraminotomy, microscopic posterior cervical foraminotomy, and more recently discovered endoscopic approaches. Percutaneous endoscopic cervical discectomy with a small single portal was developed a decade ago and has been found to lessen surgical trauma while effectively reducing compression.17 Nonetheless, accessing and working through the same small doorway offered several obstacles, including difficulty maneuvering.23
UBE decompression is a novel minimally invasive endoscopic procedure for decompressing spinal neuronal tissues. UBE with 2 portals has substantial advantages over uniportal endoscopic surgery, including a larger surgical field and greater freedom of working instruments as the viewing and working portals are separate and independent of each other. The surgeon has discrete viewing and working ports for easy maneuvering with working instruments. Continuous irrigation helps to minimize intraoperative complications, alleviates postoperative pain,24 and reduces the chance of infection.24,25 Another advantage is that this procedure allows the surgeon to utilize the same conventional instruments as open decompression techniques.
Our sample included 20 patients with a male predominance, and the most common levels involved were C5 to C6 and C6 to C7. This is consistent with previous research on the natural history of cervical spondylosis.26,27 Our study found more clinical improvement than other studies, as evidenced by improved VAS scores for arm and neck pain and NDI. At the final follow-up, the mean VAS for arm pain improved from 6.4 ± 0.7 to 0.6 ± 0.5 (92% improvement), whereas the mean VAS for neck pain improved from 3.3 ± 0.4 to 2.0 ± 0.2 (40% improvement). The NDI score improved from 23.2 ± 1.95 to 5.7 ± 0.6 (75% improvement). The clinical outcomes were similar to prior research by Park et al.28 In their series of 13 patients, Park et al found that the mean length of stay in the hospital was 2.5 days (2–5 days). Our cohort’s mean length of stay in the hospital was 1 day, which can be attributed to shorter surgical times and consequently lower usage of general anesthesia. Zheng et al29 reported on the outcomes of UBE foraminotomy combined with piezosurgery in 12 CSR patients. Instead of a rotating burr, they employed a piezosurgery instrument that uses microvibrations to cut bone precisely while avoiding neurovascular damage. Their study found that VAS and NDI scores improved after a mean follow-up of 16.8 months, indicating positive clinical outcomes. Their study found a mean operation time of 251.2 ± 14.6 minutes, approximately 4 times that of ours (64.3 ± 10.6 minutes).
There were no intraoperative complications reported in our cohort. Throughout the follow-up period, none of the patients reported persistent or worsening discomfort. None of the patients underwent revision surgery throughout the follow-up period. Possible complications documented in the literature include a dural tear, nerve root injury, increased intraoperative bleeding, epidural hematoma, and an increase in epidural pressure resulting from increased irrigating saline pressure, which can cause postoperative headache, seizures, intracranial hematoma, and blindness.30–35 These complications can be reduced by taking the following precautions during surgery:
Intraoperative bleeding: (a) Proper positioning of the patient with head up and feet down to ensure patent venous return; (b) mean arterial pressure around 90 mm Hg and heart rate <60 beats per minute; (c) use of diamond burr to reduce bone bleeding; (d) bone wax can also be used to stop persistent bone bleed; and (e) use of small tip radiofrequency probe to control epidural vessel bleeding and muscular bleeding.
Dural tear: (a) Keep the ligament flavum intact until the bone drill work is done; (b) drill work following flavectomy should be judiciously done as dust obscures clear vision; (c) Kerrison punch should be used cautiously under clear vision; (d) small dural tear can be closed with a fibril sealant or sutureless nonpenetrating clips;36,37 and (e) if the tear is large or primary repair fails, the procedure should be converted to open microscopic surgery for repair.34
Epidural hematoma: (a) Control of bleeders with radiofrequency coagulation throughout the procedure; (b) use of hemostatic agent38 (Floseal; Baxter) at the end and flush it after 2 minutes and check for any bleeders before closure; and (c) use of drain for a day or 2.
Increased epidural pressure: (a) Keep the irrigating saline pressure below 30 mm Hg and (b) keep the surgical duration to optimum as excessive and prolonged irrigation can cause meningeal irritation and headache.33,39
Nerve root injury: (a) Avoid excessive traction while retracting nerve root during discectomy; (b) careful use of burr and Kerrison punch while doing pediculotomy; and (c) small tip radiofrequency probe should be carefully used while coagulating epidural vessels near the nerve root.
Limitations
There are several limitations to this study: (1) It was a single-center retrospective study with a small sample size; (2) a brief follow-up period, making it unable to establish long-term results; (3) no radiological outcomes; (4) no comparison group. Future research should carry out a bigger multicenter prospective comparative analysis to establish the long-term outcomes of this novel technique.
Conclusion
The current study suggests that UBE decompression is a safe and effective surgical treatment option for CSR patients with good short-term clinical outcomes, shorter duration of surgery, and reduced length of hospital stay. It provides a clear and magnified view of the surgical field, as well as easy handling and manipulation of the operating equipment, reducing the risk of iatrogenic neurovascular injury. UBE minimizes the risk of postoperative instability and deterioration in sagittal parameters by avoiding iatrogenic damage to the posterior cervical musculoligamentous tissues and minimizing facet joint violation.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.