


Abstract
Background Full endoscopic spine surgery via a transforaminal approach (FESS-TFA) offers a minimally invasive approach for spinal decompression. However, it carries a risk of nerve root irritation or injury. Existing intraoperative neuromonitoring primarily provides retrospective warnings of potential nerve disturbance.
Objective To introduce the use of stimulated electromyography neuromonitoring dilators in FESS-TFA for proactive nerve protection, enhanced localization, and potential reduction in radiation exposure.
Methods This technical note describes the first use of neuromonitoring dilators in FESS-TFA. A 6-mm dilator tipped with a stimulation electrode is introduced to provide real-time directional feedback regarding nerve proximity, allowing the surgeon to actively avoid accidental injury to the exiting nerve root. With the creation of a safe tract, subsequent introduction of working instruments would theoretically reduce the risk of neural injury.
Results The technique was successfully applied in a case of T11/T12 severe spinal stenosis, facilitating safe instrument passage and nerve localization. We describe the surgical technique and provide illustrative intraoperative details.
Conclusion Neuromonitoring dilators represent a promising innovation in FESS-TFA with the potential to enhance patient safety and possibly streamline the procedure. Larger-scale studies are warranted to quantify the true impact of this technique on complication rates, operative time, and radiation exposure.
Clinical Relevance This technique highlights a significant advancement in reducing neural complications during minimally invasive spinal surgeries. By proactively preventing nerve irritation or injury and reducing radiation exposure, it contributes to optimizing surgical workflows and improving patient outcomes.
Level of Evidence 5.
Introduction
Endoscopic transforaminal decompression, also known as full endoscopic spine surgery (FESS), is an emerging technique popularized by its minimal disruption to spinal tissue, direct visualization and access to compressive pathology, and reported shorter recovery times. It has proven itself to be an effective surgical technique.1 The transforaminal approach (TFA) has been widely utilized since its introduction in 1972 by Kambin.2 However, 1 of the primary concerns of this technique is the potential risk of irritation to the dorsal root ganglia, exiting nerve root, and the furcal nerve in the foraminal area. This risk has a reported incidence of up to 2% according to a meta-analysis of complications of percutaneous endoscopic lumbar discectomy.3,4 The risk of such a complication is increased in older patients and those with severe disc degeneration.4
Efforts have been dedicated to reducing the risk of nerve root irritation and damage. Literature suggests considering open or microdiscectomy in cases where the exiting nerve root is positioned too low or if the distance between the exiting nerve root and facet is too narrow, aiming to reduce the risk of neural injury.5 Another commonly utilized approach is to use multimodal intraoperative neuromonitoring (IONM) in the form of motor, somatosensory evoked potential, and electromyography to guide the operating surgeon as to when neural irritation occurs during FESS.6,7 However, a limitation of IONM is that it provides retrospective information; the signs of neural irritation and injury will only become apparent after the damage has been done.
As such, we wish to propose the use of stimulated electromyography (EMG) neuromonitoring dilators in FESS-TFA to aid in ensuring an adequate margin of clearance from neural tissue before the surgeon proceeds to safely introduce working instruments.
Surgical Technique
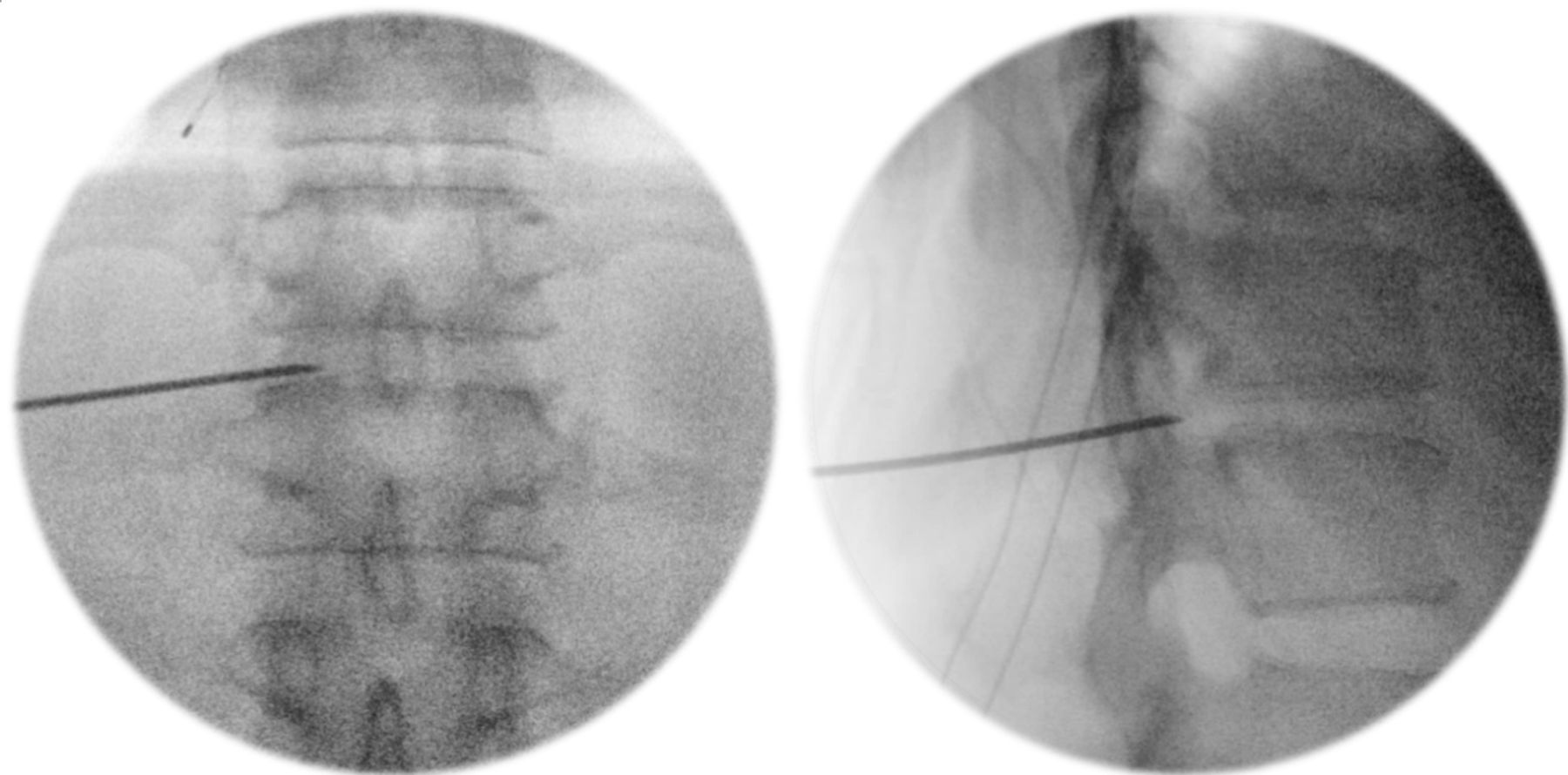
The surgery was performed with a set of full endoscopic transforaminal uniportal surgical instruments (Richard Wolf [RiWo] GmbH—VERTEBRIS lumbar transforaminal endoscope). As per standard technique, a guide needle is passed under fluoroscopic guidance to dock on at the T11 to T12 intervertebral disc, through the Kambin’s triangle. A guide wire is then passed through the guide needle and anchored in the disc (Figure 1).

Guide-needle insertion through the neural foramen onto the T11–T12 disc, confirmed with fluoroscopy.
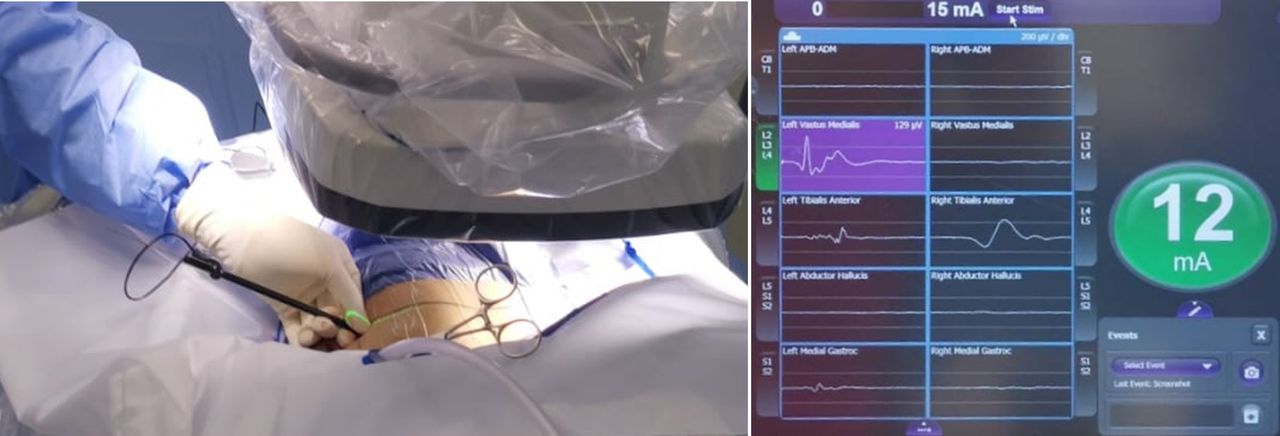
This technique involves the use of a 6-mm neuromonitoring dilator (NuVasive, Inc.—NVM5 extreme lateral interbody fusion [XLIF] dilators) that allows for dynamically evoked electromyography (Figure 2 and Table). This stimulating probe applies pulsating electrical stimuli and delivers an electrical impulse near the nerve. A recording electrode will detect a resultant muscle response of the corresponding myotome. By observing the amplitude of the EMG response detected, this technique allows us to determine the proximity of the instruments (stimulation probe and working cannula) to the nerve, providing active feedback during the initial instrumentation to adjust our trajectory and avoid nerve injury. The stimulation electrode is progressed through the neural foramen, while “real-time directionality” is achieved by rotating the dilator to direct the electrode tip toward the anticipated course of the exiting and traversing nerves. Feedback on the proximity to nervous tissue is provided as active amplitude (mA) readings.
A 6-mm neuromonitoring dilator, use adapted from the NuVasive NVM5 nerve monitoring system.
Design features of the NVM5 6-mm dilator that render it suitable for FESS.
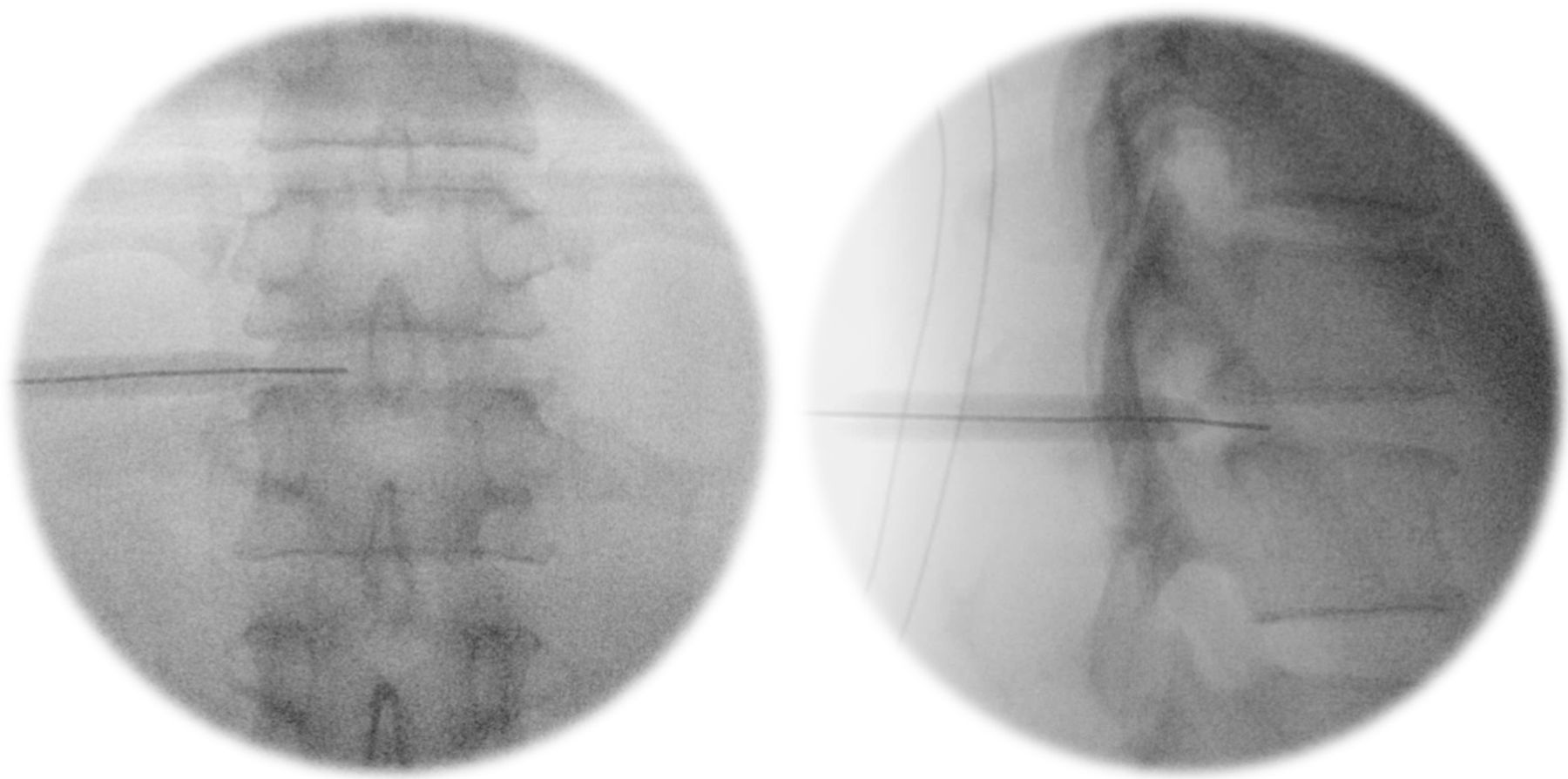
In this case, upon setting the dilator tip within the neural foramen and directing the electrode cranially toward the T11 pedicle and T11 exiting nerve root, as well as dorsally away from the disc and toward the traversing nerve root, both returned an adequate amplitude of 12 mA (Figures 3–5).

Passing the neuromonitoring dilator over the guidewire into the foramen.

Rotating the electrode tip cranially and medially to obtain readings corresponding to neural tissue proximity.

Insertion of transforaminal endoscopic instruments via the “safe tract.”
With the assurance that instrumentation is adequately positioned away from neural tissue, a standard RiWo metal dilator and cannula were gently malleted and secured onto the annulus, following which a conventional FESS-TFA decompression and discectomy was completed.
Case Presentation
An active 47-year-old woman presented with occasional radiculopathy to her lateral left thigh and calf, along with a neurogenic claudication pattern of a gluteal cramp after an average of 20 to 30 minutes of brisk walking. She suffered 6 months of progressing symptoms before presenting at our clinic, being mainly bothered by the claudication, which hampered her pastime of taking long walks for exercise.
Neurologically she retained full lower limb power and sensation, as well as normal autonomic functions. Lower limb pulses were normal without features suggestive of vascular disease.
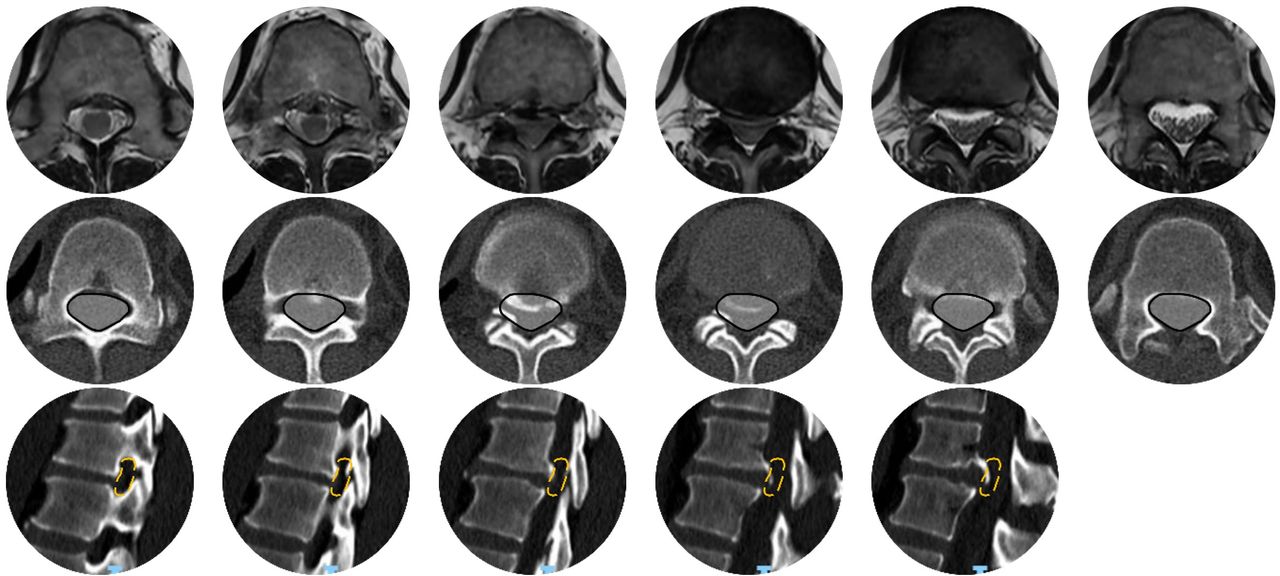
Images of her spine (Figure 6) revealed a partially calcified diffuse disc bulge causing severe spinal canal stenosis, indenting on the conus as well as contributing to bilateral lateral recess stenosis at T11 to T12. There was no other appreciable significant stenosis in the rest of her spine.

Images showing a T11/T12 partially calcified disc causing spinal canal stenosis. Top row: Magnetic resonance imaging axial cuts. Middle row: Corresponding computed tomography (CT) axial cuts. Bottom row: CT sagittal cuts (left).
Despite a trial of nonoperative management, the patient’s symptoms persisted for several months, and surgical intervention was discussed. Posterior decompression with far lateral access and potential facet resection requiring instrumentation and fusion was discussed; however, due to work commitments and the wish to avoid downtime, patient was keen for FESS-TFA decompression of the right side, accepting potential futility and secondary surgery to undergo a less invasive procedure. The distortion due to the partial calcifications was of some concern, which was attempted to be addressed with the technique described above.
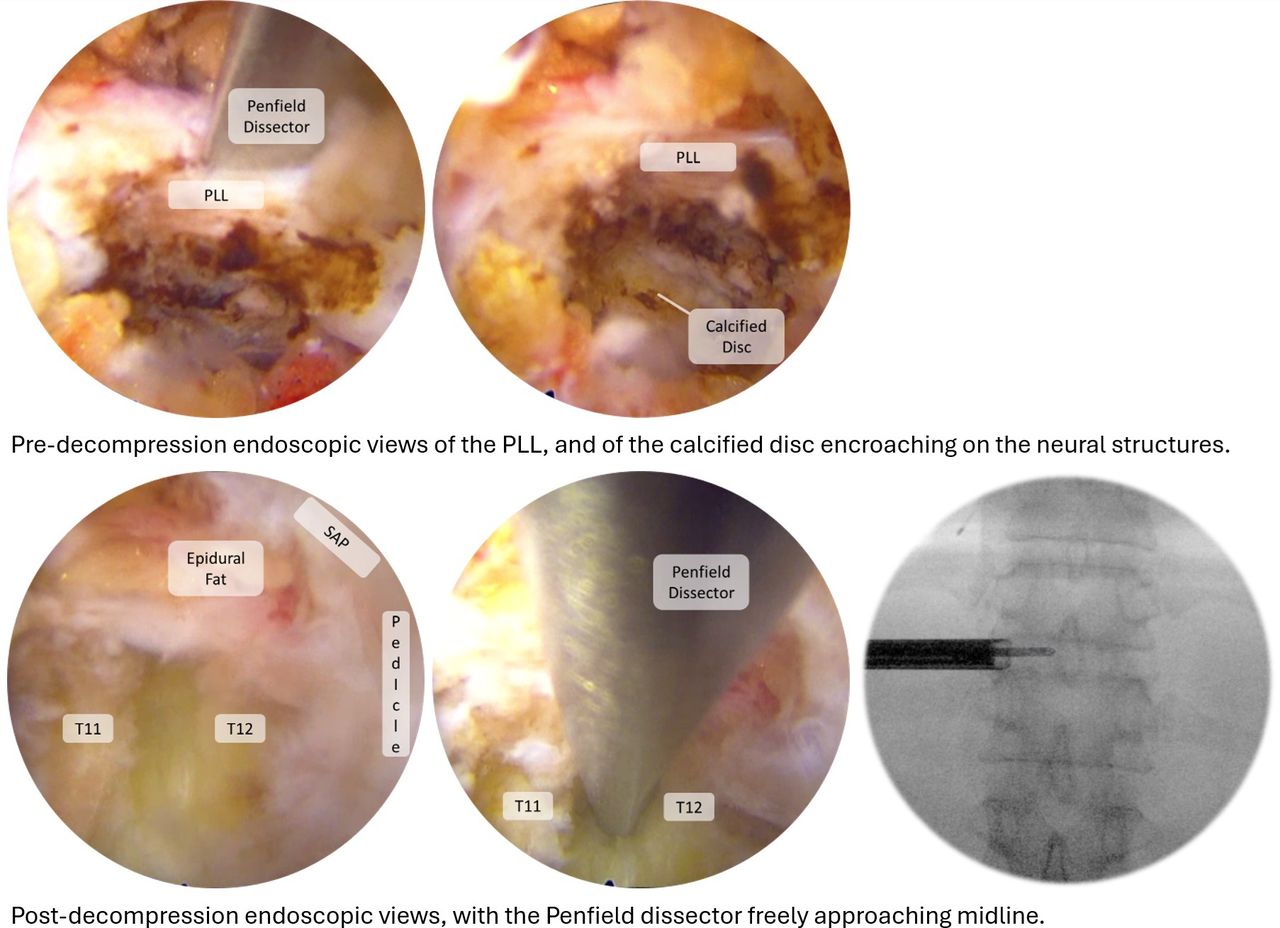
The patient underwent a right T11/T12 transforaminal FESS with modifications as described above and illustrated in Figure 7. Intraoperative monitoring EMG activity was evoked from the anterolateral abdominal musculature (rectus and transversus abdominis).8,9 Postoperatively, the patient had no neurological injury and was able to return to her desired lifestyle of participating in prolonged brisk walking without any radicular symptoms or claudication.

Endoscopic views pre- and postdecompression. Top: Predecompression endoscopic views of the posterior longitudinal ligament (PLL) and of the calcified disc encroaching on the neural structures. Bottom: Postdecompression endoscopic views, with the Penfield dissector freely approaching midline.
Discussion
The use of neuromonitoring dilators in FESS-TFA represents a novel, largely unexplored approach with the potential to optimize the safety and efficiency of this procedure. Our technical note documents the first use of this strategy to proactively avoid nerve root irritation and injury. Traditionally, the procedure involves the insertion of a fluoroscopy-guided wire followed by nonaugmented dilators, with IONM primarily indicating potential nerve disturbances after they might have occurred.6,10,11 In contrast, neuromonitoring dilators offer the advantage of proactive nerve protection. By providing real-time feedback on nerve proximity, they allow the surgeon to adjust instrument placement accordingly, instead of reacting retrospectively to injury caused. This technique may be particularly useful considering that IONM has shown that 72.7% of patients experienced compression of the exiting nerve root’s DRG during initial transforaminal placement of the working cannula.6
Moreover, neuromonitoring dilators can enhance intraoperative localization. Their dynamic feedback assists in precise identification of the nerve root and helps delineate the extent of foraminal stenosis. This enhanced visualization translates to multiple potential benefits, including streamlined surgical workflow and potentially reduced time spent meticulously navigating near critical neural structures. This follows principles similar to the neuromonitoring probe and finger electrodes used for XLIF cases to reduce their rate of neural injury.12–14
An additional potential advantage of neuromonitoring dilators is a possible reduction of radiation exposure. By providing continuous feedback on instrument position, they could decrease the need for repeated fluoroscopic imaging during surgery, minimizing radiation for both the patient and surgical team.
While further research is needed to fully quantify these benefits, this technique signals a promising refinement of the FESS-TFA approach. Larger-scale studies will be crucial in determining the impact of neuromonitoring dilators on complication rates, operative time, and cost-effectiveness. These studies will help determine whether the potential advantages of this technique justify its integration into routine FESS-TFA practice.
Conclusion
This technical note showcases the first use of neuromonitoring dilators in FESS. With this new technique, we hope that a shorter surgical time along with a lower risk of nerve root damage can be achieved.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.