


Abstract
The lateral transpsoas approach to lumbar interbody fusion has gained widespread adoption for a variety of indications. This approach to the interbody space allows for a favorable fusion environment, disc and neuroforaminal height restoration, and powerful alignment correction. Despite its minimally invasive nature, this procedure carries unique risks, the most severe of which include bowel injury, major vascular injury, and lumbosacral plexopathy. This poses a marked learning curve and requires rigorous attention to detail in technique. In this review, we provide a detailed description of our approach to preoperative imaging, patient positioning, and surgical technique, with an emphasis on patient safety and evidence-based decision-making. A brief description of intraoperative neuromonitoring techniques follows. The lateral transpsoas approach to interbody fusion has demonstrated reliable outcomes in regard to fusion rates, pain and function, and deformity correction, all across a widespread variety of lumbar spine pathologies. Here, we depict techniques, pearls, and pitfalls that are critical for any surgeon considering whether to add this technique to their practice.
- lumbar interbody fusion
- extreme lateral interbody fusion
- XLIF
- minimally invasive spine surgery
- degenerative disease
- low back pain
Introduction
In 2006, Ozgur et al published a technical report on a novel lumbar interbody fusion technique performed via a lateral approach passing through retroperitoneal fat and the psoas major muscle.1 This procedure was subsequently coined the extreme lateral interbody fusion or XLIF (NuVasive, Inc, San Diego, CA). At the time of that report, surgical candidates were those with axial lower back pain secondary to degenerative disc disease without severe central canal stenosis. They reported no complications in their series of 13 patients who had promising short-term outcomes. Over the past 2 decades, XLIF has gained widespread adoption for a variety of indications and continues to demonstrate reliable outcomes.2 Given the early positive track record associated with this minimally invasive technique and its utility in fusion constructs of various lengths and complexity, XLIF is an increasingly important tool in the spine surgeon’s armamentarium. The purpose of this review is to introduce the indications, benefits, and risks of XLIF followed by a detailed surgical technique guide based on our experience.
Indications and Benefits
In its original description, XLIF was implemented in a series of patients with axial lower back pain related to degenerative disc disease.1 Indications for the lateral transpsoas interbody fusion have subsequently expanded to further include degenerative spondylolisthesis, isthmic spondylolisthesis, lumbar radiculopathy secondary to foraminal stenosis, lumbar spinal stenosis with neurogenic claudication, recurrent lumbar disc herniation, adjacent segment disease, and spinal deformity correction.3–5 Further expansions of the lateral retroperitoneal approach have resulted in the implementation of the transpsoas technique for lateral corpectomy used in the treatment of fractures, oncologic processes, and infections. The lateral transpsoas approach is indicated to address these pathologies from L1 to L5. Anatomic limitations including the lumbar plexus and the iliac crest limit viability to access L5-S1, while approaches more cephalad to L1 are typically accomplished with a lateral retropleural approach.
The lateral transpsoas approach allows for the placement of an interbody cage that is wide in the coronal plane, increasing endplate-to-implant contact and improving force distribution. This theoretically improves the fusion environment while decreasing subsidence risk. The approach allows for the preservation of the anterior longitudinal ligament (ALL) and the posterior longitudinal ligament as well as much of the annulus, creating a stable mechanical environment for alignment correction and disc height restoration via ligamentotaxis. Ligamentotaxis has been demonstrated to facilitate indirect decompression of the spinal canal and neuroforamina.5 Contrarily, the approach can also involve ALL release for powerful anterior column realignment. The lateral transpoas procedure is unique in its ability to achieve these benefits through a minimally invasive technique, typically involving a small incision, and is associated with decreased blood loss, operative time, postoperative pain, and hospital length of stay when compared to more traditional approaches to interbody fusion.6,7
Risks and Complications
The lateral transpsoas approach also carries several risks, the most severe of which include bowel injury, major vascular injury, and lumbosacral plexopathy. Over the past decades, surgical techniques have evolved to minimize these risks.
Anatomic studies and clinical observation have demonstrated approach-related risks to the lumbar plexus, ilioinguinal, iliohypogastric, genitofemoral, lateral femoral cutaneous, and subcostal nerves.8 The true incidence of these complications may be limited by underreporting and lack of a standardized definition of each unique complication, creating a wide range of reported risks. Anterior thigh pain is one of the most reported complications, ranging from 25% to 39%, with most cases resolving within 90 days of the procedure.9,10 Meta-analysis has reported variable incidences of postoperative neurological deficits, ranging from 0% to 36% for motor deficits and 0% to 75% for sensory issues.11 Neurological deficits are most commonly associated with injury to the lumbar plexus in varying forms and severities of neurapraxia or more rarely axonotmesis. Motor deficits associated with these injuries typically improve over the course of 3 to 6 months.12 Even in the absence of neurapraxia, transient hip flexion weakness secondary to psoas trauma is commonly experienced, and this symptom typically resolves over the course of about 2 weeks.13 Most of the aforementioned complications seem to resolve within 90 days of surgery. Sensory deficits usually follow this trend; however, 1 series reported 5 of 8 patients to have persistent sensory deficits at 10.5 months postoperatively.14 Considering the highly variable reported incidences of complications, thorough discussion and informed consent with knowledge of all anticipated consequences are essential aspects of preoperative planning with patients.
Iatrogenic bowel injury and perforation have been reported at rates from 0.03% to 12.5% in the literature with these injuries requiring emergent general surgery consultation.15 Ipsilateral psoas hematoma and even contralateral psoas muscle hematoma can be observed.16,17 While rare in the transpsoas approach, vascular injury has been reported in the literature at a rate of up to 0.4% and can be fatal.18
Due to unique regional anatomy, the lateral transpsoas approach at L4-L5 has been purported to be associated with an increased risk of approach-related complications. The lumbar plexus migrates progressively anteriorly as it moves more distally, while vascular structures tend to move more posteriorly, effectively closing down the “safe zone” corridor as has been demonstrated in both magnetic resonance imaging (MRI) and cadaveric studies.19,20 Literature on complications at L4-L5 has been somewhat heterogeneous. In a 2019 retrospective cohort study, addressing L4-L5 levels via lateral transpsoas approach was associated with significantly greater rates of motor deficits than lateral approaches not addressing L4-L5 (13% vs 5.5%).21 However, a more recent study by Nolte et al reported similar rates of low-approach–related complications between lateral transpsoas approaches at L4-L5 and more cephalad levels, with no statistically significant difference in hip flexor weakness between the cohorts (53.5% L4-L5 vs 37.5% L1-L4).22 The above complications are likely also a function of psoas retraction time, highlighting the need for an efficient approach. Bendersky et al reviewed 107 patients undergoing the transpoas approach and had no lumbar plexopathies when retraction time was less than 20 minutes per level.23
Rigorous attention to detail during preoperative planning, intraoperative positioning, and surgical technique serves to minimize these risks, especially when approaching the more distal lumbar levels.
Technique
Preoperative Imaging
Preoperative evaluation should begin with an assessment of plain radiographs to determine the position of the iliac crest relative to the operative level. This is most easily assessed on a lateral view, but the anteroposterior view can also provide insight into approach laterality/viability in cases of significant coronal tilt of the operative level. Bending films can provide additional insight into crest position if available. Additionally, axial imaging, including CT and MRI, can be utilized to assess the position of the iliac crest relative to the operative level as these recumbent images can serve as a better proxy for intraoperative alignment in comparison to standing films. Having determined the mechanical viability of the lateral approach relative to the iliac crest, attention should turn toward an assessment of critical neurovascular structures.
Axial cuts on MRI are most useful for identifying vascular structures such as the aorta, inferior vena cava, and common iliac vessels, which run adjacent to the ventral surface of the ALL. These views also facilitate assessment of the lumbar plexus as it arises from the foramina of L2 through L4. Position of the plexus should be identified on T2 and T1 sequences to assess the width of the approach corridor. A study by Regev et al reviewed 100 MRI studies to determine general safe corridors with respect to the adjacent neurovascular structures.24 They found a narrowing of the safe surgical corridor from the L1-L2 level to the L4-L5 level. This narrowing occurs as the retroperitoneal vessels move posterior and lateral with respect to the vertebral body, while lumbar plexus nerve position shifts anterior, with an abrupt change at the L4-L5 level. It was also determined that rotational changes associated with scoliosis result in anatomic distortions, including a more posterior lumbar plexus and a more posterior great vessel position, particularly along the curve concavity.24
MRI is also very useful in determining the size and position of the psoas muscle. Patients with lumbosacral transitional vertebrae may have an anteriorly shifted psoas muscle placing the lumbar plexus at higher risk.25 It should be noted, however, that important neurovascular structures may shift during lateral positioning. Deukmedjian et al obtained MRIs in both supine and lateral positions in 10 healthy volunteers and found that in the left lateral decubitus position, the inferior vena cava shifted 1.2 cm anteriorly and 1 cm to the left with these values increasing rostrally. In the right lateral decubitus, the inferior vena cava translated 6 mm to the right. The aorta had limited change in location in either position, while the psoas muscle did not shift appreciably but became flatter.26
Prior to proceeding with a lateral approach, a safe corridor between the major vascular structures and the lumbar plexus should be identified. Factors such as an anteriorly positioned psoas muscle, an anteriorly positioned plexus within the psoas muscle, or posteriorly/laterally positioned vascular structures mandate that the surgeon consider of other potential approaches.
Positioning
Patient positioning and operating room set-up are critical for safe completion of a lateral transpsoas procedure. Typically, a regular operative table in reverse “diving-board” position is utilized. After neuromonitoring lead placement, the patient is then turned to a lateral decubitus position with the break of the operative table positioned between the greater trochanter and the iliac crest. For improved access to more cephalad spinal levels, the break should be moved closer to the iliac crest, while for access to L4-L5, the break should be closer to the greater trochanter. An axillary roll is placed under the axilla of the downside to avoid brachial plexus compression, take pressure off the humeral head, and allow for respiratory expansion. A pad should be placed under the down leg to protect the peroneal nerve. The hips should be flexed about 30° and the knees flexed to about 45° to alleviate tension on the iliopsoas and the lumbar plexus. The arms are forward flexed to 90° and placed in gentle elbow flexion and neutral abduction using either a table-mounted arm holder or a stack of pillows. Bolsters consisting of rolled blankets with reverse wrapped tape can be placed anteriorly and posteriorly for further stabilization. Pelvic rotation is then set with the application of circumferential tape positioned proximal to the greater trochanter on the patient and distal to the table break on the bed (Figure 1). The thoracic spine is then gently secured with circumferential taping in a similar fashion with care to avoid over-constriction (Figure 2). To provide further stability and facilitate greater positioning control, the pelvis and legs are then further taped and secured to the bed. Padding should be applied at the upside peroneal nerve and ankle. The tape then runs from the greater trochanter down the thigh, loops around the distal end of the bed, travels parallel to the leg again crossing the knee, and then loops back around the bed over the top of the previously applied tape, just proximal to the trochanter (Figures 3 and 4).

The pelvis is secured with circumferential tape that is affixed to the bed distal to the bed break. Tape should be proximal to the greater trochanter and distal to the iliac crest to avoid draping out of any planned incisions.

The chest is secured with circumferential taping.

The pelvis and legs are further secured with circumferential taping.

The pelvis and legs are further secured with circumferential taping (view from above).
The table is then broken to improve access between the 12th rib and the iliac crest (Figure 5). One must balance the need for improved access by breaking the bed with the risk of increasing tension on the psoas and lumbar plexus.

The table is then “broken” to improve access between the 12th rib and the iliac crest. The amount of table break is greater for levels more cephalad or more caudal due to these structures.
The C-arm is then brought in to obtain a perfect anteroposterior (AP) view (Figure 6). All imaging adjustments should be performed with adjustment of the patient rather than the C-arm such that true orthogonal position of the target level is achieved. A true AP view is confirmed by visualizing the spinous processes midline, bisecting the pedicles, and ensuring perfectly linear endplates. In cases with segmental rotation, the caudal vertebra of the target level is typically utilized to confirm rotation, though careful study of preoperative axial imaging can provide additional insight. Malrotation on the AP view leads to either anterior or posterior trajectories of instrumentation, which is amplified with longer retractor blades and in larger patients. This can lead to implant malposition, neurological injury, or catastrophic vascular injury. As such, achieving and maintaining a perfect AP view is 1 of the most important steps of the procedure. Any time that a subsequent AP view is obtained, the surgeon should be confirming that rotation has not changed. After achieving a perfect AP, the C-arm is rotated to the lateral view. Trendelenberg positioning is then used to achieve a perfect lateral view with linear endplates, a linear cortex, and superimposed pedicles.

After securing the patient to the bed, the bed is rotated to obtain a perfect anteroposterior fluoroscopic image. C-arm position is impacted by room orientation and size. Having the intensifier on the posterior reduces surgeon radiation but comes at the cost of ergonomic challenges working around the larger portion of the C-arm.
A radiopaque guidewire can then be used to mark the skin at the anterior and posterior margins of the vertebrae. The angle of the disc space should be marked and extended anteriorly and posteriorly to subsequently assist in retractor alignment. In cases addressing multiple levels, the disc space of each level should be marked in this fashion, and the decision should then be made to make either multiple incisions or 1 longer, oblique incision (Figure 7).

Example of marking for L3-L4 and L4-L5. Each disc space angle is marked more broadly, in addition to anterior and posterior aspects of the vertebral body and superior and inferior endplates.
Approach
The previously demarcated skin incision is then carried out and sharp dissection is carried out down to the level of the fascia of the abdominal wall. This fascia is then released in line with the skin incision. The external oblique, internal oblique, and transversalis fascia are then bluntly split, allowing visualization of the underlying retroperitoneal fat. This can be performed with either a blunt-tipped hemostat, a Kocher clamp, or a Metzenbaum scissors. Use of sharp dissection or electrocautery should be avoided as the iliohypogastric and ilioinguinal nerves can be encountered in the layer between the oblique muscles. Upon visualization of the retroperitoneal fat, blunt finger dissection should be utilized to palpate the iliac crest, the 12th rib, or both, depending on regional anatomy. These landmarks serve to confirm the correct dissection layer. Manual palpation should then allow for release of retroperitoneal fat by swiping a finger cephalad and caudal along the posterior wall. The iliolumbar ligament, the quadratus lumborum, and the transverse processes can be palpated posteriorly. As the retroperitoneal fat is further released anteriorly, the longitudinal fibers of the psoas muscle can be palpated.
Two-Incision Technique
In its original description, the lateral transpsoas approach also utilizes a posterior counterincision positioned just lateral to the paraspinal muscles, allowing entry to the retroperitoneal space more posteriorly. A finger is used to then similarly palpate the psoas muscle and retroperitoneal anatomy. An initial dilator is then seated on the psoas muscle as confirmed by palpation through this posterior incision. The initial dilator is then ready to be advanced into the psoas musculature under live electromyography (EMG) and fluoroscopic visualization.
Single-Incision Docking Short Technique
If planning a single-incision approach, the initial dilator can be rested on top of the palpated psoas. Sequential dilators are then placed without advancement into the psoas. Short retractor blades are affixed and the retractor is then seated over these dilators, remaining superficial to the psoas muscle. The retractor can then be opened in the retroperitoneal space, allowing for direct visualization of the psoas muscle (Figure 8). Any residual retroperitoneal fat can then be bluntly swept anteriorly with the use of an endoscopic Kittner sponge. If the psoas is not able to be directly visualized, the retractor should be removed, and further blunt dissection and palpation of the psoas should be carried out. Once the psoas is directly visualized, the psoas fascia can be bluntly released, thus allowing for direct visualization of the longitudinally oriented fibers. Live EMG can then be implemented to identify the lumbar plexus. The initial dilator can then be gently advanced into the psoas muscle under direct visualization. The superficially positioned retractor can then be removed (Figure 9).

Example of shallow docking technique. After seating the initial dilator on top of the psoas and dilating up to the retractor, the retractor is then opened superficially to the muscle, allowing the surgeon direct visualization of the muscle prior to piercing the psoas with the initial dilator. An endoscopic Kittner sponge can be used to clear any retroperitoneal fat if there is an obscured view of the psoas.

After the initial dilator is seated in the psoas muscle under electromyography stimulation, the superficially positioned retractor is then removed.
Psoas Dilation and Retractor Positioning
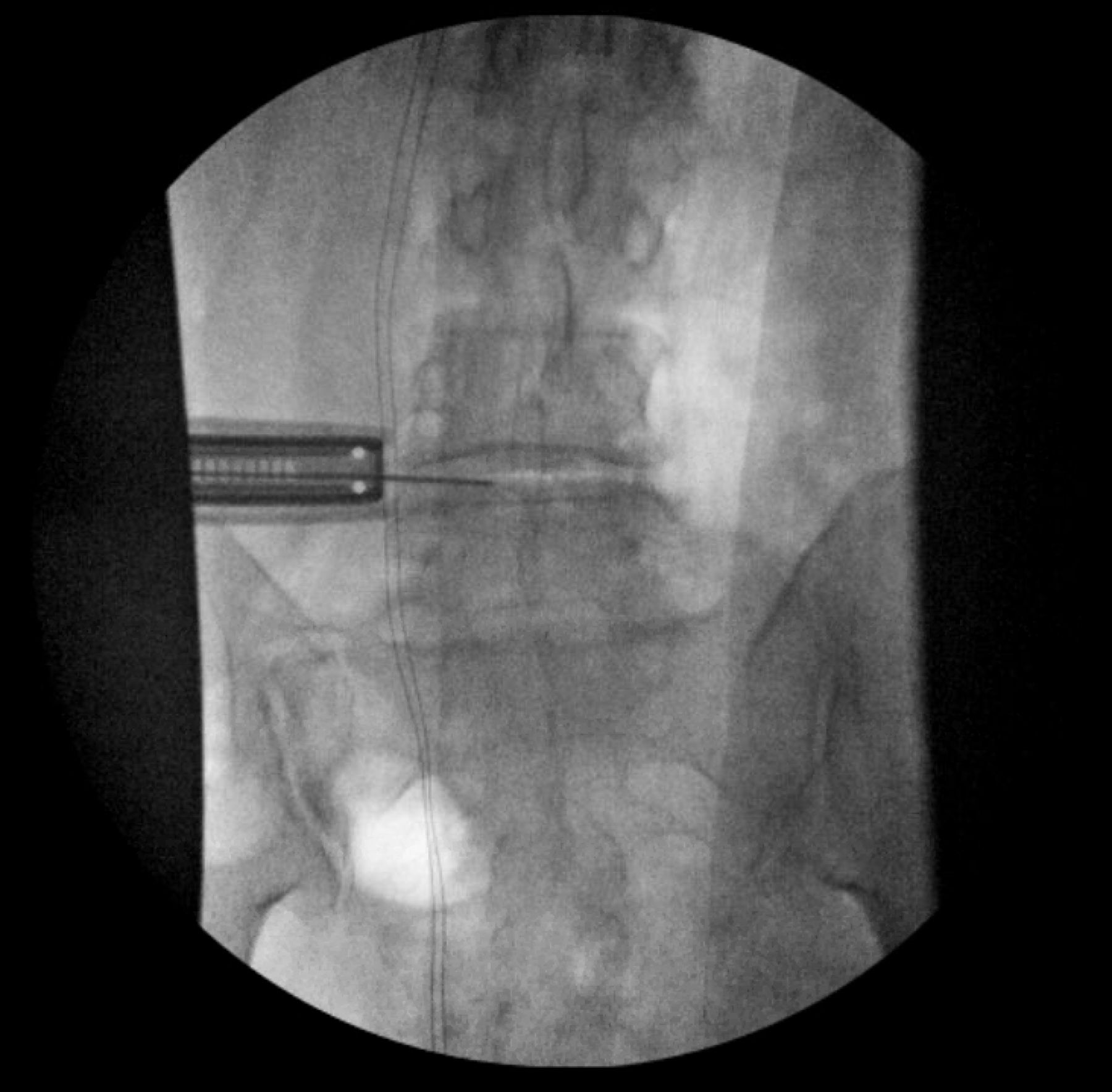
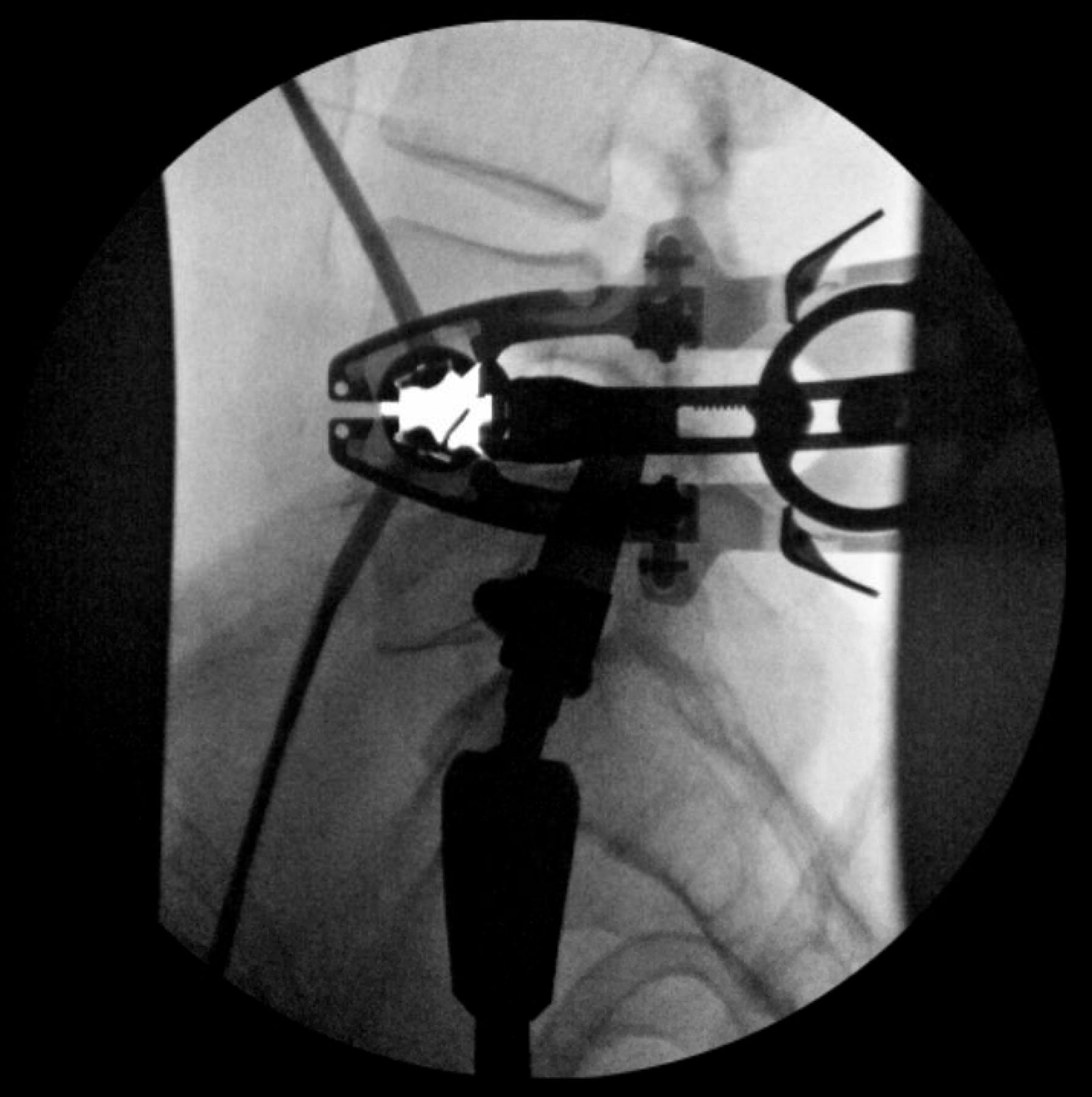
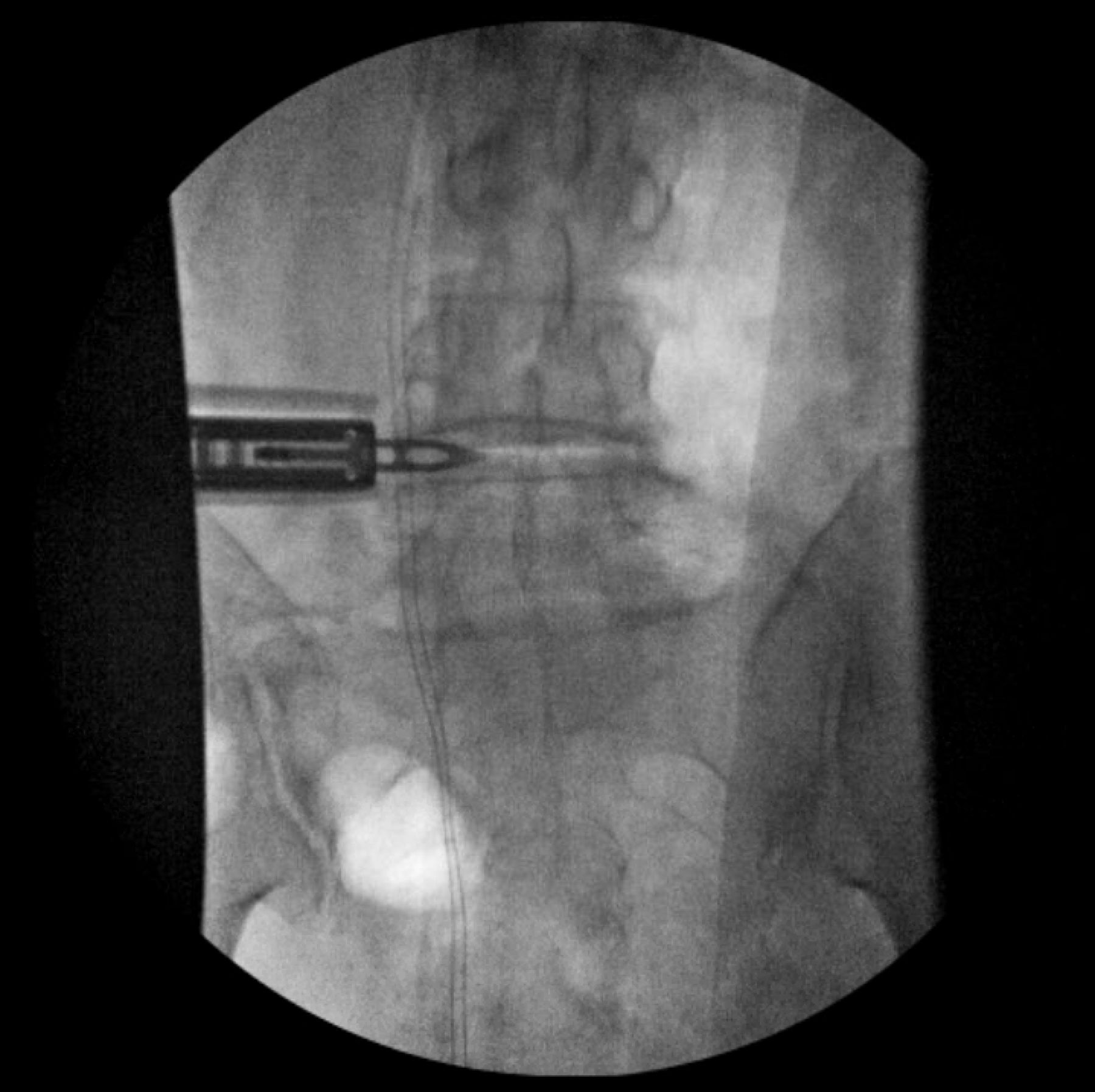
Following advancement of the initial dilator into the psoas under directional EMG, it is held in position with a radiolucent clamp. The initial dilator is then positioned over the disc space under lateral fluoroscopy, generally targeting just posterior to the middle of the disc space, though this can be more specifically chosen if aiming to lock the anterior blade and open the retractor posteriorly vs locking the posterior blade and opening the retractor anteriorly (Figure 10). A guidewire is then advanced into the disc space to fix the position of the initial dilator. Sequential dilators are then placed under live, directional EMG to confirm clearance of the posterior lying lumbar plexus (Figure 11). The retractor is then placed, ensuring that the retractor handles are parallel to the floor and in line with the previous disc space marking during localization. The position of the retractor is then fine-tuned under lateral views to confirm rotation and neutral anteroposterior trajectory. A lateral view can confirm appropriate position over the disc space. Dilators can then be removed, leaving the guidewire in place as a point of reference. At this point, the retractor can be slightly opened to allow visualization of the spine (Figures 12 and 13). The field should be stimulated with EMG to confirm the absence of neurological structures. The lumbosacral plexus should then be identified posterior to the posterior retractor blade with the EMG to confirm its position.

Position of the initial dilator is confirmed at the level of the disc space on lateral fluoroscopy.

Sequential dilation through the psoas is performed under live, directional electromyography. The position of the plexus should be identified posteriorly.

Orientation of the retractor is confirmed relative to the disc space on anteroposterior view.

Orientation of the retractor is confirmed relative to the disc space on the lateral view. The retractor is slightly opened to allow electromyography stimulation along the anterior aspect of the posterior blade prior to shim placement.
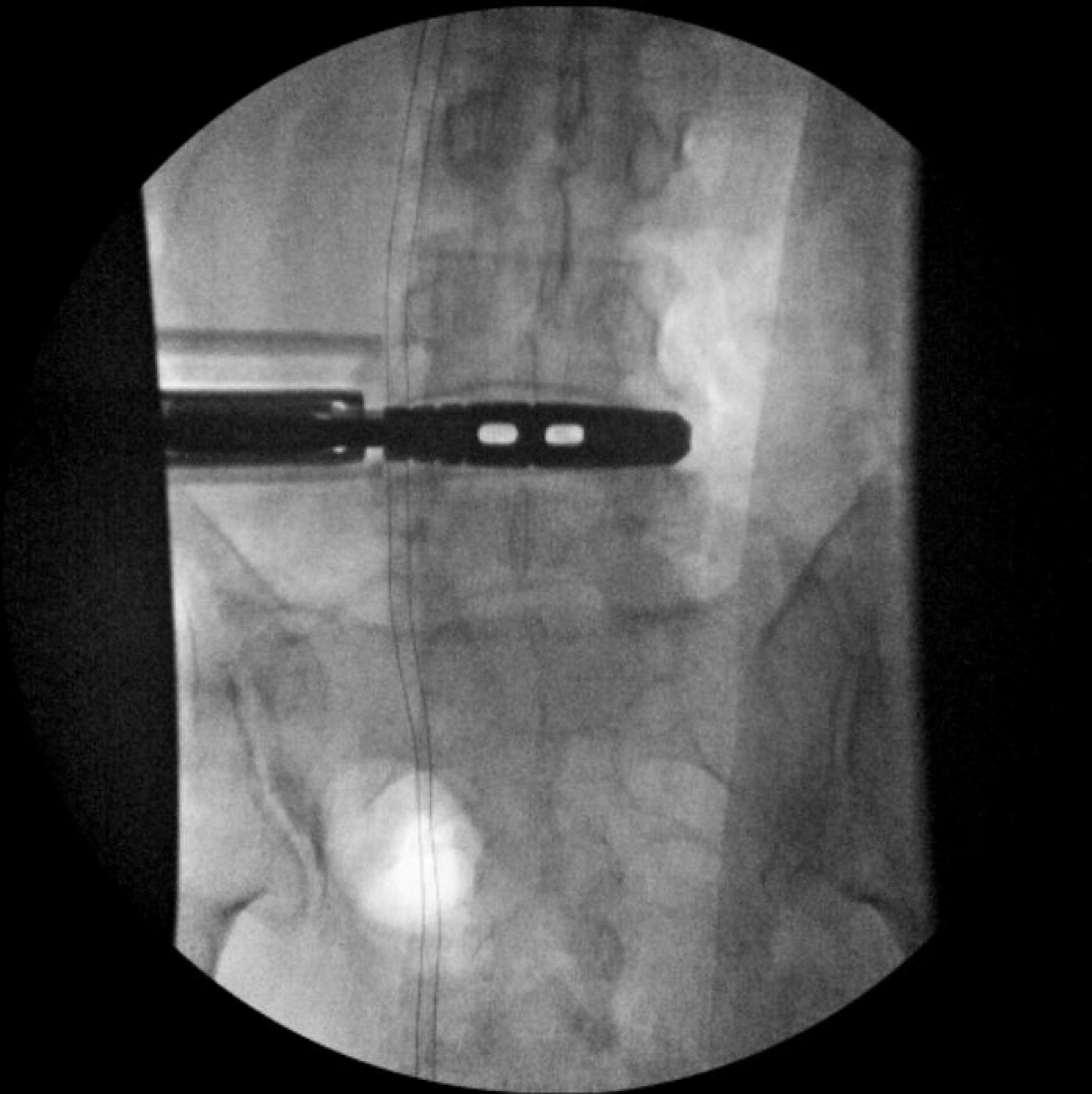
At this point, following confirmation of the position of the retractor on lateral imaging, the surgeon can either elect to place a disc shim or continue without shim placement. Shims offer the benefit of retractor stability and soft tissue protection. Additionally, in cases of a high iliac crest or a low 12th rib, shims offer a fixed point against which the retractor can be tilted, allowing for improved retractor position with minimized retractor creep. However, care must be taken during their placement, as anteriorly malpositioned shims can cause vascular injury, and posteriorly malpositioned shims can cause neurological injury. Additionally, cephalocaudally malpositioned shims can result in vertebral body bleeding or segmental vessel injury. If opening the retractor anteriorly, the posterior shim should be placed first. If opening the retractor posteriorly, the anterior shim should be placed first. The field at the site of shim entry should be stimulated with EMG to confirm the absence of neurological structures at the shim insertion site. A stimulation value of less than 8 mA should cause the surgeon to pause and consider further blunt dissection prior to shim placement. The shim should be placed under AP fluoroscopy (Figure 14).

The shim is then placed under anteroposterior fluoroscopy.
The retractor should then be opened to facilitate disc space visualization and implant placement. Attempts should be made to minimize retractor opening beyond that necessary to visualize the target disc space and allow placement of the planned anteroposterior diameter implant to minimize lumbar plexus traction and psoas irritation (Figure 15).

The retractor is then opened. The position of the anterior and posterior blades as well as the retractor orientation/angle should be noted to allow for further visual landmarks of the operative “safe zone.”
Disc Space Preparation and Implant Placement
At this point, a systematic approach should be adopted with surgical instruments sequentially lined up for each step below to facilitate an efficient procedure. Studies have correlated the duration of retractor expansion with postoperative complications and outcomes with the general consensus that poorer outcomes and greater complication rates are seen with retractor dilation times greater than 20 minutes.27 Efficient setup and workflow can reduce retraction time while still achieving appropriate and safe disc space preparation.
The C-arm is positioned to obtain an AP view. An annulotomy is performed with a long-handled knife. A Cobb elevator is then passed along each endplate in a position perfectly perpendicular to the floor of the room (neutral AP angulation due to patient positioning). The Cobb or blunt distractor is used to then release the contralateral annulus with care taken to avoid plunging through the contralateral psoas. The preoperative MRI should be used to assess for the vascular location on the contralateral side to the approach to ensure the safe trajectory of instruments through the lateral disc space. The authors recommend initiating this portion of the procedure first with an 18-mm Cobb prior to expansion to a 22- or 23-mm Cobb if desired. In some cases, a mallet is necessary to pass the Cobb and release the contralateral annulus, but the need for excessive force should cause pause as these can indicate malrotation causing contact with the ALL or posterior longitudinal ligament or can indicate inadvertent endplate violation. In these cases, scrutiny of radiographs is recommended prior to proceeding. A discectomy is then carried out with use of a pituitary and a curette. A Kerrison can be used to widen the annulotomy window and improve direct visualization of the disc space. Following the initial preparation of the space, a ring curette can be used to further remove disc material and endplate cartilage.
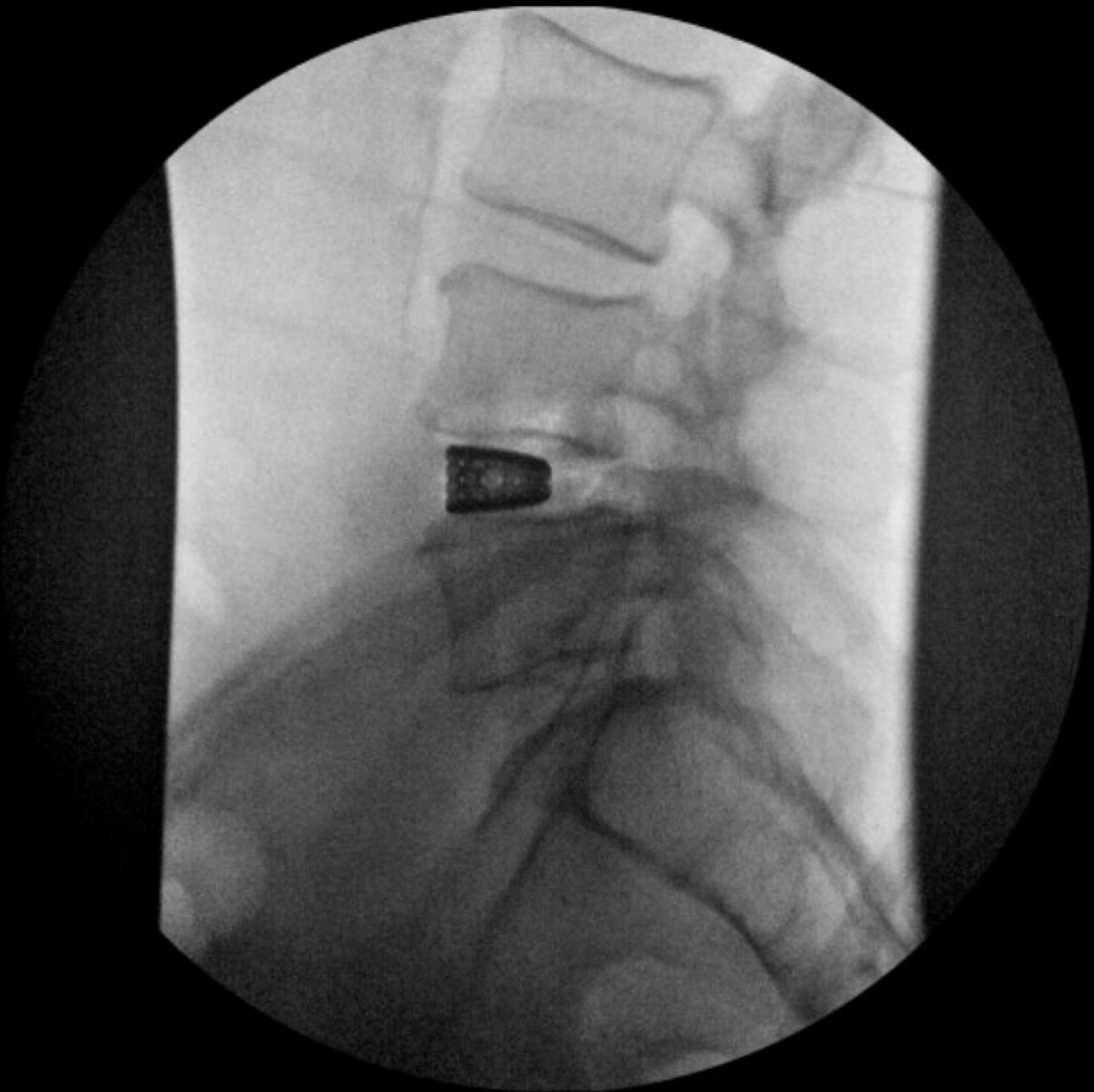
At this point, trialing can begin. Trials can be sequentially increased in height and width as accommodated by patient anatomy. If at any point during trialing there is a significant reduction in the amount of force necessary to place the implant, the surgeon should be concerned about iatrogenic ALL release. This can be assessed via gentle rotation of each trial to confirm continued resistance or by direct palpation anteriorly with a blunt-tipped instrument. In the event of ALL release, a lateral plate should be available to provide support with screws placed into each adjacent vertebral body. Preoperative imaging should serve to provide targets for implant height and lordosis. Ideally, the implant should rest on the lateral apophyseal ring of the endplate without extending beyond to maximize mechanical support while limiting psoas irritation. Prior to implant selection, a lateral view should be obtained with a trial in place to confirm appropriate position and afford an opportunity for correction if necessary (Figures 16 and 17). A final implant is then selected. During the time necessary for the surgical technician to prepare the implant, disc preparation should be finalized again with use of curettes and rongeurs as the dilation of the trials will often improve disc space access. Prior to implant placement, the disc space should be flushed with irrigation. The final cage is then impacted under direct and flurosocopic guidance. The insertion handle is then removed, hemostasis maintained with bipolar cautery and hemostatic agents, and topical antibiotic applied. Disc shims are then removed if placed. AP and lateral fluoroscopic images are taken confirming appropriate position of the implant (Figures 18–20).

Trialing is performed under anteroposterior fluoroscopy. After determining the appropriate implant length and height, position of the trial is confirmed on lateral imaging.

After determining the appropriate implant length and height on the anteroposterior view, position of the trial is confirmed on lateral imaging.

The final implant is then placed on anteroposterior fluoroscopy.

The insertion handle is removed, and final position of the implant is confirmed on the anteroposterior view.

Final position of the implant is confirmed on the lateral view.
Closure
The retractor is then partially collapsed and slowly removed under direct visualization. Any brisk bleeding should be controlled with bipolar electrocautery and hemostatic agents prior to complete retractor removal. Final AP and lateral views should be obtained at this point. The lateral abdominal wall fascia is then tightly closed, and superficial layers are closed in a layered fashion.
Navigated and Robotic Assistance
The advent of navigation and robotic technology has been applied to the lateral transpsoas technique, with studies showing early clinical safety and efficacy. Sinkov et al demonstrated the use of preoperatively planned pedicle screw trajectories using a navigation system software allowing accurate screw placement in the lateral decubitus position through posterior percutaneous incisions, prior to proceeding with the lateral transpsoas approach as described above.28 This allows for accurate posterior fixation to be achieved without having to re-position the patient prone, which can increase operative time, as well as intra-abdominal blood pressure leading to higher blood loss. Urakawa et al describe the use of intraoperative navigation during the lateral transpsoas approach itself, using navigation to plan their incision, guide their approach trajectory during muscle splitting and retroperitoneal entry, localize the disc space, and position the first dilator accurately.29 Performing all of these steps under navigation reduces the need for fluoroscopy and decreasing radiation dose.28,29
Neuromonitoring
Intraoperative neuromonitoring techniques warrant mention given their widespread use in lateral transpsoas approaches given the importance of protection of the lumbar plexus. Alluri et al reviewed the current literature on the use of intraoperative EMG, motor-evoked potentials (MEPs), and somatosensory-evoked potentials (SSEPs) and their limitations when used in isolation, suggesting a multimodal monitoring approach to be safer.30
Triggered EMG determines the distance of the lumbar plexus from the dilators while they are being stimulated. The benefit to a directional EMG system is the ability to determine where the dilator or retractor lies in relation to the lumbar plexus. In an ideal scenario, stimulating the probe signals the presence of lumbar plexus nerves only posterior to the dilator, signifying that the retractor will be placed anterior these neural structures. If there is a signal that is circumferential to the stimulated dilator, this may indicate that the current dilation tract is within an axilla of the lumbar plexus, in which case the approach should be shifted anteriorly in most cases. EMG does have limitations such as a low specificity and inability to determine whether true nerve injury is developing, increasing the risk of nerve injury when used as the sole neuromonitoring technique.31
Riley et al demonstrated that in patients who underwent XLIF with both EMG and MEPs monitoring, patients were less likely to have postoperative neurological deficits.32 MEPs may be able to monitor quadriceps innervation from lumbar plexus nerves, thus improving the ability to detect neurological injury. A trained neuromonitoring team is usually required to interpret MEPs, which must also be assessed relative to preoperative baseline MEPs.
Finally, saphenous nerve SSEP monitoring has been described as an adjunct method to identify impending femoral nerve injury. Silverstein et al noted SSEP changes during retractor expansion in 5 of their 46 patients undergoing XLIF.33 They did not report any false negatives while using this method. Three of the patients with SSEP changes did have postoperative femoral nerve deficits, despite these patients not having any intraoperative EMG changes, underlying the potential utility in multimodal monitoring techniques.33
Outcomes
Over the course of its more widespread utilization, the lateral transpsoas approach has demonstrated considerably good outcomes. Reliable fusion rates of 83% to 95% at 1-year follow-up have been reported in the literature.9,34 Meta-analyses have reported significant improvements in leg and back visual analog scale scores as well as the Oswestry Disability Index scores at 1-year follow-up.2 Disc height, lumbar lordosis, and segmental lordosis were also significantly corrected postoperatively in these studies as well as in the analysis of the implementation of the technique in the treatment of degenerative scoliosis.2,35–37 Multiple studies have reported on outcomes for a variety of specific pathologies, but this is beyond the scope of this article.
Conclusion
The lateral transpsoas approach has proven to be a utilitarian approach for a wide variety of pathologies. The minimally invasive nature of the technique not only affords significant advantages but also comes with the potential for significant complications that must be minimized through rigorous preoperative planning and precise intraoperative technique. Consequently, appropriate training with exposure to techniques, pearls, and pitfalls during the early learning curve of this procedure is critical for any surgeon considering adding the lateral transpsoas technique to their practice.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosures T. Barrett Sullivan reports consulting for Kato Medical and teaching/consulting for Orthofix Seaspine. Frank M. Phillips reports royalties from Globus and SI Bone; consulting for Globus, Stryker, Medtronic, Spine Art, and Augmedics; and serving on the Board of Directors/Advisory Board (stock/options) for Globus, SI Bone, Mainstay, Spinal Simplicity, Augmedics, and Providence.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2025 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.